Martin Torp Rahbek, Søren Andreas Just, Kasper Bruun Kristensen, Hussam Mahmoud Sheta, Jesper Hallas, Anton Pottegård, Lars Christian Lund
{"title":"开始服用胰高血糖素样肽 1 受体激动剂后嗜酸性粒细胞增多症的风险增加:利用丹麦健康登记进行的对称性分析。","authors":"Martin Torp Rahbek, Søren Andreas Just, Kasper Bruun Kristensen, Hussam Mahmoud Sheta, Jesper Hallas, Anton Pottegård, Lars Christian Lund","doi":"10.1111/joim.20025","DOIUrl":null,"url":null,"abstract":"<p>Glucagon-like peptide 1 receptor agonists (GLP1-RA) are increasingly used in the treatment of Type 2 diabetes and as antiobesity drugs. Cases of hypereosinophilic syndrome (HES) following initiation of GLP1-RA have been reported [<span>1</span>]. HES is defined by eosinophil counts of 1.5 × 10<sup>9</sup>/L or greater and related end-organ damage [<span>2</span>]. Because these events are too rare to be detected in randomized controlled trials, we aimed to quantify the association between GLP1-RA initiation and incident hypereosinophilia (HE) using real-world data.</p><p>Leveraging nationwide Danish prescription [<span>3</span>] and laboratory data [<span>4</span>], we conducted a sequence symmetry analysis (SSA) investigating the occurrence of HE following initiation of GLP1-RA and for comparison sodium–glucose co-transporter 2 inhibitors (SGLT2i) and dipeptidyl peptidase 4 inhibitors (DPP4i) [<span>5</span>].</p><p>The SSA compares the occurrence of HE during a symmetric time window before and after initiation of the drug of interest. If there is no association between drug initiation and HE, we would expect HE to occur equally often during both windows. However, if GLP1-RA use increases eosinophil counts, we would expect HE to occur more frequently after initiation. The sequence ratio (SR) is calculated as the number of HE events after drug initiation divided by the number of HE events before drug initiation and corresponds to the incidence rate ratio obtained in the corresponding cohort study [<span>6</span>]. If the rate of HE is increased after initiation of GLP1-RA compared to the period before initiation, we would expect an SR above 1.</p><p>We identified all individuals who initiated a GLP1-RA, SGLT2i or DPP4i (Appendix) between 1 June 2015 and 31 May 2024 and obtained eosinophil counts of 1.5 × 10<sup>9</sup>/L or greater within the last 180 days before the drug initiation, or within the first 180 days after. Observed SRs were adjusted for temporal trends in HE [<span>5</span>]. In subgroup analyses, we evaluated semaglutide and other GLP1-RAs separately, as well as Ozempic and Wegovy. For sensitivity analyses, we calculated SRs for observation windows of 90 and 365 days and with mild (≥0.5–1.5 × 10<sup>9</sup>/L) and massive eosinophilia (≥5 × 10<sup>9</sup>/L) as outcomes. Finally, we used a thrombocyte count below 50 × 10<sup>9</sup>/L as a negative control outcome.</p><p>The study was approved by the institutional data protection board at the University of Southern Denmark and the Danish Health Data Authority (Project number FSEID-00006047). Ethical approval is not needed in Denmark for studies based purely on registry data.</p><p>We identified 213,521 individuals who initiated a GLP1-RA among whom 245 had HE within 1 year of drug initiation. The median age was 54 years (interquartile range [IQR] 42–63), 49% were female and median year of initiation of GLP1-RA was 2022 (IQR 2021–2023<i>)</i>. Of these, 193 individuals had HE after drug initiation, and 52 individuals had HE before drug initiation, yielding an SR of 3.83 (95% confidence interval [CI] 2.84–5.24). Among initiators of SGLT2i and DPP4i, we found SRs of 0.76 (<i>N</i> = 108/146, CI 0.59–0.97) and 0.89 (<i>N</i> = 68/76, CI 0.64–1.23).</p><p>In subgroup analyses, SRs for semaglutide, other GLP1-RAs, Wegovy and Ozempic were similar to results for all GLP1-RAs combined (Fig. 1). The outcome mild eosinophilia yielded an SR of 1.08 for GLP1-RA initiators (<i>N</i> = 1207/1136, CI 1.0–1.18). For massive eosinophilia, we observed 13 events after GLP1-RA initiation and less than 5 events before initiation. Analyses with shorter and longer observation windows yielded elevated SRs (SR 3.87, CI 2.62–5.85 and 2.50 [1.97–3.18]). For the negative-control outcomes, we found for GLP1-RA, SGLT2i and DPP4i, respectively, SRs of 1.64 (<i>N</i> = 44/27, CI 1.02–2.66), SR of 1.28 (<i>N</i> = 118/93, CI 0.98–1.68) and SR of 0.84 (<i>N</i> = 75/89, CI 0.62–1.15) after initiation. <b>Fig</b>. <b>S1</b> shows a steep increase in HE during the first 3 months after GLP1-RA initiation, which was not observed for SGLT2i or DPP4i initiators.</p><p>In this nationwide study, we found that HE is three times more likely to occur after initiation of GLP1-RAs compared to the period prior to initiation. This finding was specific to GLP1-RAs and not observed for other antidiabetic drugs. Albeit the negative control outcome generated a result that was non-null for GLP1-RAs, results for the negative control outcome were much closer to 1.0 compared to the main analysis and were compatible with the results for SGLT2i. Thus, our study provides evidence of a temporal association between the initiation of GLP1-RAs and HE. The main limitation of our study is that the outcome was biochemically defined HE and not end-organ damage due to HE. Another important limitation is that the study population only included individuals who initiated GLP1-RA and had an eosinophil count measured. Larger studies are needed to quantify the potential association between GLP1-RAs and clinically manifest HES.</p><p>The data underlying this article cannot be shared publicly due to Danish privacy regulations. Danish data are available to authorized researchers after application to the Danish Health Data Authority (https://sundhedsdatastyrelsen.dk).</p><p>The analytical source code can be obtained from https://gitlab.sdu.dk/lclund/glp1-hes/. A protocol was registered prior to data analysis and is available at https://osf.io/sabzk.</p><p>Martin Torp Rahbek and Lars Christian Lund had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Lars Christian Lund, Martin Torp Rahbek, Anton Pottegård, Jesper Hallas and Kasper Bruun Kristensen conceptualized the study. Søren Andreas Just and Hussam Mahmoud Sheta provided important input to the methodology and interpretation. Lars Christian Lund performed the data analysis. Martin Torp Rahbek drafted the original manuscript, and all authors critically revised the manuscript and approved the final version for publication. Martin Torp Rahbek attests that Anton Pottegård, Jesper Hallas, Lars Christian Lund, Søren Andreas Just, Kasper Bruun Kristensen and Hussam Mahmoud Sheta meet authorship criteria and that no others meeting the criteria have been omitted.</p><p>LCL reports participation in research projects funded by Menarini Pharmaceuticals and LEO Pharma, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the current work. JH reports participation in post-authorization safety studies funded by Novo Nordisk with money paid to his employer and with no personal fees involved. AP reports participation in research projects funded by Alcon, Almirall, Astellas, Astra-Zeneca, Boehringer-Ingelheim, Novo Nordisk, Servier and LEO Pharma, all regulator-mandated phase IV-studies, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the work reported in this article. HMS is currently employed by Novo Nordisk but did not have any affiliation with Novo Nordisk at the time of data analysis and manuscript draft writing. MTR, KBK and SAJ report no conflicts of interest.</p><p>None.</p>","PeriodicalId":196,"journal":{"name":"Journal of Internal Medicine","volume":"296 6","pages":"527-530"},"PeriodicalIF":9.2000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.20025","citationCount":"0","resultStr":"{\"title\":\"Increased risk of hypereosinophilia following initiation of glucagon-like peptide 1 receptor agonist: A symmetry analysis using the Danish health registries\",\"authors\":\"Martin Torp Rahbek, Søren Andreas Just, Kasper Bruun Kristensen, Hussam Mahmoud Sheta, Jesper Hallas, Anton Pottegård, Lars Christian Lund\",\"doi\":\"10.1111/joim.20025\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Glucagon-like peptide 1 receptor agonists (GLP1-RA) are increasingly used in the treatment of Type 2 diabetes and as antiobesity drugs. Cases of hypereosinophilic syndrome (HES) following initiation of GLP1-RA have been reported [<span>1</span>]. HES is defined by eosinophil counts of 1.5 × 10<sup>9</sup>/L or greater and related end-organ damage [<span>2</span>]. Because these events are too rare to be detected in randomized controlled trials, we aimed to quantify the association between GLP1-RA initiation and incident hypereosinophilia (HE) using real-world data.</p><p>Leveraging nationwide Danish prescription [<span>3</span>] and laboratory data [<span>4</span>], we conducted a sequence symmetry analysis (SSA) investigating the occurrence of HE following initiation of GLP1-RA and for comparison sodium–glucose co-transporter 2 inhibitors (SGLT2i) and dipeptidyl peptidase 4 inhibitors (DPP4i) [<span>5</span>].</p><p>The SSA compares the occurrence of HE during a symmetric time window before and after initiation of the drug of interest. If there is no association between drug initiation and HE, we would expect HE to occur equally often during both windows. However, if GLP1-RA use increases eosinophil counts, we would expect HE to occur more frequently after initiation. The sequence ratio (SR) is calculated as the number of HE events after drug initiation divided by the number of HE events before drug initiation and corresponds to the incidence rate ratio obtained in the corresponding cohort study [<span>6</span>]. If the rate of HE is increased after initiation of GLP1-RA compared to the period before initiation, we would expect an SR above 1.</p><p>We identified all individuals who initiated a GLP1-RA, SGLT2i or DPP4i (Appendix) between 1 June 2015 and 31 May 2024 and obtained eosinophil counts of 1.5 × 10<sup>9</sup>/L or greater within the last 180 days before the drug initiation, or within the first 180 days after. Observed SRs were adjusted for temporal trends in HE [<span>5</span>]. In subgroup analyses, we evaluated semaglutide and other GLP1-RAs separately, as well as Ozempic and Wegovy. For sensitivity analyses, we calculated SRs for observation windows of 90 and 365 days and with mild (≥0.5–1.5 × 10<sup>9</sup>/L) and massive eosinophilia (≥5 × 10<sup>9</sup>/L) as outcomes. Finally, we used a thrombocyte count below 50 × 10<sup>9</sup>/L as a negative control outcome.</p><p>The study was approved by the institutional data protection board at the University of Southern Denmark and the Danish Health Data Authority (Project number FSEID-00006047). Ethical approval is not needed in Denmark for studies based purely on registry data.</p><p>We identified 213,521 individuals who initiated a GLP1-RA among whom 245 had HE within 1 year of drug initiation. The median age was 54 years (interquartile range [IQR] 42–63), 49% were female and median year of initiation of GLP1-RA was 2022 (IQR 2021–2023<i>)</i>. Of these, 193 individuals had HE after drug initiation, and 52 individuals had HE before drug initiation, yielding an SR of 3.83 (95% confidence interval [CI] 2.84–5.24). Among initiators of SGLT2i and DPP4i, we found SRs of 0.76 (<i>N</i> = 108/146, CI 0.59–0.97) and 0.89 (<i>N</i> = 68/76, CI 0.64–1.23).</p><p>In subgroup analyses, SRs for semaglutide, other GLP1-RAs, Wegovy and Ozempic were similar to results for all GLP1-RAs combined (Fig. 1). The outcome mild eosinophilia yielded an SR of 1.08 for GLP1-RA initiators (<i>N</i> = 1207/1136, CI 1.0–1.18). For massive eosinophilia, we observed 13 events after GLP1-RA initiation and less than 5 events before initiation. Analyses with shorter and longer observation windows yielded elevated SRs (SR 3.87, CI 2.62–5.85 and 2.50 [1.97–3.18]). For the negative-control outcomes, we found for GLP1-RA, SGLT2i and DPP4i, respectively, SRs of 1.64 (<i>N</i> = 44/27, CI 1.02–2.66), SR of 1.28 (<i>N</i> = 118/93, CI 0.98–1.68) and SR of 0.84 (<i>N</i> = 75/89, CI 0.62–1.15) after initiation. <b>Fig</b>. <b>S1</b> shows a steep increase in HE during the first 3 months after GLP1-RA initiation, which was not observed for SGLT2i or DPP4i initiators.</p><p>In this nationwide study, we found that HE is three times more likely to occur after initiation of GLP1-RAs compared to the period prior to initiation. This finding was specific to GLP1-RAs and not observed for other antidiabetic drugs. Albeit the negative control outcome generated a result that was non-null for GLP1-RAs, results for the negative control outcome were much closer to 1.0 compared to the main analysis and were compatible with the results for SGLT2i. Thus, our study provides evidence of a temporal association between the initiation of GLP1-RAs and HE. The main limitation of our study is that the outcome was biochemically defined HE and not end-organ damage due to HE. Another important limitation is that the study population only included individuals who initiated GLP1-RA and had an eosinophil count measured. Larger studies are needed to quantify the potential association between GLP1-RAs and clinically manifest HES.</p><p>The data underlying this article cannot be shared publicly due to Danish privacy regulations. Danish data are available to authorized researchers after application to the Danish Health Data Authority (https://sundhedsdatastyrelsen.dk).</p><p>The analytical source code can be obtained from https://gitlab.sdu.dk/lclund/glp1-hes/. A protocol was registered prior to data analysis and is available at https://osf.io/sabzk.</p><p>Martin Torp Rahbek and Lars Christian Lund had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Lars Christian Lund, Martin Torp Rahbek, Anton Pottegård, Jesper Hallas and Kasper Bruun Kristensen conceptualized the study. Søren Andreas Just and Hussam Mahmoud Sheta provided important input to the methodology and interpretation. Lars Christian Lund performed the data analysis. Martin Torp Rahbek drafted the original manuscript, and all authors critically revised the manuscript and approved the final version for publication. Martin Torp Rahbek attests that Anton Pottegård, Jesper Hallas, Lars Christian Lund, Søren Andreas Just, Kasper Bruun Kristensen and Hussam Mahmoud Sheta meet authorship criteria and that no others meeting the criteria have been omitted.</p><p>LCL reports participation in research projects funded by Menarini Pharmaceuticals and LEO Pharma, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the current work. JH reports participation in post-authorization safety studies funded by Novo Nordisk with money paid to his employer and with no personal fees involved. AP reports participation in research projects funded by Alcon, Almirall, Astellas, Astra-Zeneca, Boehringer-Ingelheim, Novo Nordisk, Servier and LEO Pharma, all regulator-mandated phase IV-studies, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the work reported in this article. HMS is currently employed by Novo Nordisk but did not have any affiliation with Novo Nordisk at the time of data analysis and manuscript draft writing. MTR, KBK and SAJ report no conflicts of interest.</p><p>None.</p>\",\"PeriodicalId\":196,\"journal\":{\"name\":\"Journal of Internal Medicine\",\"volume\":\"296 6\",\"pages\":\"527-530\"},\"PeriodicalIF\":9.2000,\"publicationDate\":\"2024-10-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.20025\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Internal Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/joim.20025\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/joim.20025","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Increased risk of hypereosinophilia following initiation of glucagon-like peptide 1 receptor agonist: A symmetry analysis using the Danish health registries
Glucagon-like peptide 1 receptor agonists (GLP1-RA) are increasingly used in the treatment of Type 2 diabetes and as antiobesity drugs. Cases of hypereosinophilic syndrome (HES) following initiation of GLP1-RA have been reported [1]. HES is defined by eosinophil counts of 1.5 × 109/L or greater and related end-organ damage [2]. Because these events are too rare to be detected in randomized controlled trials, we aimed to quantify the association between GLP1-RA initiation and incident hypereosinophilia (HE) using real-world data.
Leveraging nationwide Danish prescription [3] and laboratory data [4], we conducted a sequence symmetry analysis (SSA) investigating the occurrence of HE following initiation of GLP1-RA and for comparison sodium–glucose co-transporter 2 inhibitors (SGLT2i) and dipeptidyl peptidase 4 inhibitors (DPP4i) [5].
The SSA compares the occurrence of HE during a symmetric time window before and after initiation of the drug of interest. If there is no association between drug initiation and HE, we would expect HE to occur equally often during both windows. However, if GLP1-RA use increases eosinophil counts, we would expect HE to occur more frequently after initiation. The sequence ratio (SR) is calculated as the number of HE events after drug initiation divided by the number of HE events before drug initiation and corresponds to the incidence rate ratio obtained in the corresponding cohort study [6]. If the rate of HE is increased after initiation of GLP1-RA compared to the period before initiation, we would expect an SR above 1.
We identified all individuals who initiated a GLP1-RA, SGLT2i or DPP4i (Appendix) between 1 June 2015 and 31 May 2024 and obtained eosinophil counts of 1.5 × 109/L or greater within the last 180 days before the drug initiation, or within the first 180 days after. Observed SRs were adjusted for temporal trends in HE [5]. In subgroup analyses, we evaluated semaglutide and other GLP1-RAs separately, as well as Ozempic and Wegovy. For sensitivity analyses, we calculated SRs for observation windows of 90 and 365 days and with mild (≥0.5–1.5 × 109/L) and massive eosinophilia (≥5 × 109/L) as outcomes. Finally, we used a thrombocyte count below 50 × 109/L as a negative control outcome.
The study was approved by the institutional data protection board at the University of Southern Denmark and the Danish Health Data Authority (Project number FSEID-00006047). Ethical approval is not needed in Denmark for studies based purely on registry data.
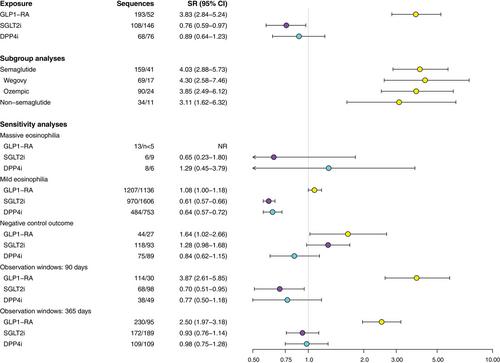
We identified 213,521 individuals who initiated a GLP1-RA among whom 245 had HE within 1 year of drug initiation. The median age was 54 years (interquartile range [IQR] 42–63), 49% were female and median year of initiation of GLP1-RA was 2022 (IQR 2021–2023). Of these, 193 individuals had HE after drug initiation, and 52 individuals had HE before drug initiation, yielding an SR of 3.83 (95% confidence interval [CI] 2.84–5.24). Among initiators of SGLT2i and DPP4i, we found SRs of 0.76 (N = 108/146, CI 0.59–0.97) and 0.89 (N = 68/76, CI 0.64–1.23).
In subgroup analyses, SRs for semaglutide, other GLP1-RAs, Wegovy and Ozempic were similar to results for all GLP1-RAs combined (Fig. 1). The outcome mild eosinophilia yielded an SR of 1.08 for GLP1-RA initiators (N = 1207/1136, CI 1.0–1.18). For massive eosinophilia, we observed 13 events after GLP1-RA initiation and less than 5 events before initiation. Analyses with shorter and longer observation windows yielded elevated SRs (SR 3.87, CI 2.62–5.85 and 2.50 [1.97–3.18]). For the negative-control outcomes, we found for GLP1-RA, SGLT2i and DPP4i, respectively, SRs of 1.64 (N = 44/27, CI 1.02–2.66), SR of 1.28 (N = 118/93, CI 0.98–1.68) and SR of 0.84 (N = 75/89, CI 0.62–1.15) after initiation. Fig. S1 shows a steep increase in HE during the first 3 months after GLP1-RA initiation, which was not observed for SGLT2i or DPP4i initiators.
In this nationwide study, we found that HE is three times more likely to occur after initiation of GLP1-RAs compared to the period prior to initiation. This finding was specific to GLP1-RAs and not observed for other antidiabetic drugs. Albeit the negative control outcome generated a result that was non-null for GLP1-RAs, results for the negative control outcome were much closer to 1.0 compared to the main analysis and were compatible with the results for SGLT2i. Thus, our study provides evidence of a temporal association between the initiation of GLP1-RAs and HE. The main limitation of our study is that the outcome was biochemically defined HE and not end-organ damage due to HE. Another important limitation is that the study population only included individuals who initiated GLP1-RA and had an eosinophil count measured. Larger studies are needed to quantify the potential association between GLP1-RAs and clinically manifest HES.
The data underlying this article cannot be shared publicly due to Danish privacy regulations. Danish data are available to authorized researchers after application to the Danish Health Data Authority (https://sundhedsdatastyrelsen.dk).
The analytical source code can be obtained from https://gitlab.sdu.dk/lclund/glp1-hes/. A protocol was registered prior to data analysis and is available at https://osf.io/sabzk.
Martin Torp Rahbek and Lars Christian Lund had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Lars Christian Lund, Martin Torp Rahbek, Anton Pottegård, Jesper Hallas and Kasper Bruun Kristensen conceptualized the study. Søren Andreas Just and Hussam Mahmoud Sheta provided important input to the methodology and interpretation. Lars Christian Lund performed the data analysis. Martin Torp Rahbek drafted the original manuscript, and all authors critically revised the manuscript and approved the final version for publication. Martin Torp Rahbek attests that Anton Pottegård, Jesper Hallas, Lars Christian Lund, Søren Andreas Just, Kasper Bruun Kristensen and Hussam Mahmoud Sheta meet authorship criteria and that no others meeting the criteria have been omitted.
LCL reports participation in research projects funded by Menarini Pharmaceuticals and LEO Pharma, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the current work. JH reports participation in post-authorization safety studies funded by Novo Nordisk with money paid to his employer and with no personal fees involved. AP reports participation in research projects funded by Alcon, Almirall, Astellas, Astra-Zeneca, Boehringer-Ingelheim, Novo Nordisk, Servier and LEO Pharma, all regulator-mandated phase IV-studies, all with funds paid to the institution where he was employed (no personal fees) and with no relation to the work reported in this article. HMS is currently employed by Novo Nordisk but did not have any affiliation with Novo Nordisk at the time of data analysis and manuscript draft writing. MTR, KBK and SAJ report no conflicts of interest.
期刊介绍:
JIM – The Journal of Internal Medicine, in continuous publication since 1863, is an international, peer-reviewed scientific journal. It publishes original work in clinical science, spanning from bench to bedside, encompassing a wide range of internal medicine and its subspecialties. JIM showcases original articles, reviews, brief reports, and research letters in the field of internal medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


