{"title":"基于分泌素的药物对永久性新生儿糖尿病患者血糖控制的长期影响。","authors":"Ayaka Oshiro, Ryoichiro Aotani, Wakako Sakamoto, Takanari Kitazono, Toshiaki Ohkuma","doi":"10.1210/jcemcr/luae188","DOIUrl":null,"url":null,"abstract":"<p><p>Permanent neonatal diabetes mellitus (PNDM) is a genetic disorder, characterized by a decrease in endogenous insulin secretion. Therefore, exogenous insulin supplementation plays a central role in controlling glycemia. Although adding a sulfonylurea can help to discontinue insulin, discontinuation is sometimes difficult when the sulfonylurea is administered at older ages. A 24-year-old woman with longstanding PNDM who had poor glycemic control using insulin (47 U/day) and high-dose glibenclamide (0.6 mg/kg/day), had successfully discontinued insulin after initiating the dipeptidyl peptidase-4 inhibitor sitagliptin (50 mg/day). Additionally, hemoglobin A1c levels decreased by 4.8%. Double dosing of sitagliptin and subsequent switching to the glucagon-like peptide-1 receptor agonist semaglutide (0.25 mg/week followed by 0.5 mg/week) further decreased hemoglobin A1c values, with graded improvements in endogenous insulin secretion. There were no episodes of hypoglycemia during which glibenclamide was titrated down from 0.6 to 0.4 mg/kg/day. Intra- and inter-day glucose variability as assessed by continuous glucose monitoring was also improved. In patients with PNDM, administration and dose escalation of incretin-based drugs, in addition to a high-dose sulfonylurea, could be a useful treatment strategy. This strategy may be helpful for discontinuing insulin, downtitrating sulfonylureas, and subsequent achievement of better glycemic control regarding long-term stability and short-term variability.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"2 11","pages":"luae188"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11487289/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-Term Effects of Incretin-Based Drugs on Glycemic Control in Permanent Neonatal Diabetes.\",\"authors\":\"Ayaka Oshiro, Ryoichiro Aotani, Wakako Sakamoto, Takanari Kitazono, Toshiaki Ohkuma\",\"doi\":\"10.1210/jcemcr/luae188\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Permanent neonatal diabetes mellitus (PNDM) is a genetic disorder, characterized by a decrease in endogenous insulin secretion. Therefore, exogenous insulin supplementation plays a central role in controlling glycemia. Although adding a sulfonylurea can help to discontinue insulin, discontinuation is sometimes difficult when the sulfonylurea is administered at older ages. A 24-year-old woman with longstanding PNDM who had poor glycemic control using insulin (47 U/day) and high-dose glibenclamide (0.6 mg/kg/day), had successfully discontinued insulin after initiating the dipeptidyl peptidase-4 inhibitor sitagliptin (50 mg/day). Additionally, hemoglobin A1c levels decreased by 4.8%. Double dosing of sitagliptin and subsequent switching to the glucagon-like peptide-1 receptor agonist semaglutide (0.25 mg/week followed by 0.5 mg/week) further decreased hemoglobin A1c values, with graded improvements in endogenous insulin secretion. There were no episodes of hypoglycemia during which glibenclamide was titrated down from 0.6 to 0.4 mg/kg/day. Intra- and inter-day glucose variability as assessed by continuous glucose monitoring was also improved. In patients with PNDM, administration and dose escalation of incretin-based drugs, in addition to a high-dose sulfonylurea, could be a useful treatment strategy. This strategy may be helpful for discontinuing insulin, downtitrating sulfonylureas, and subsequent achievement of better glycemic control regarding long-term stability and short-term variability.</p>\",\"PeriodicalId\":73540,\"journal\":{\"name\":\"JCEM case reports\",\"volume\":\"2 11\",\"pages\":\"luae188\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-10-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11487289/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCEM case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1210/jcemcr/luae188\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luae188","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Long-Term Effects of Incretin-Based Drugs on Glycemic Control in Permanent Neonatal Diabetes.
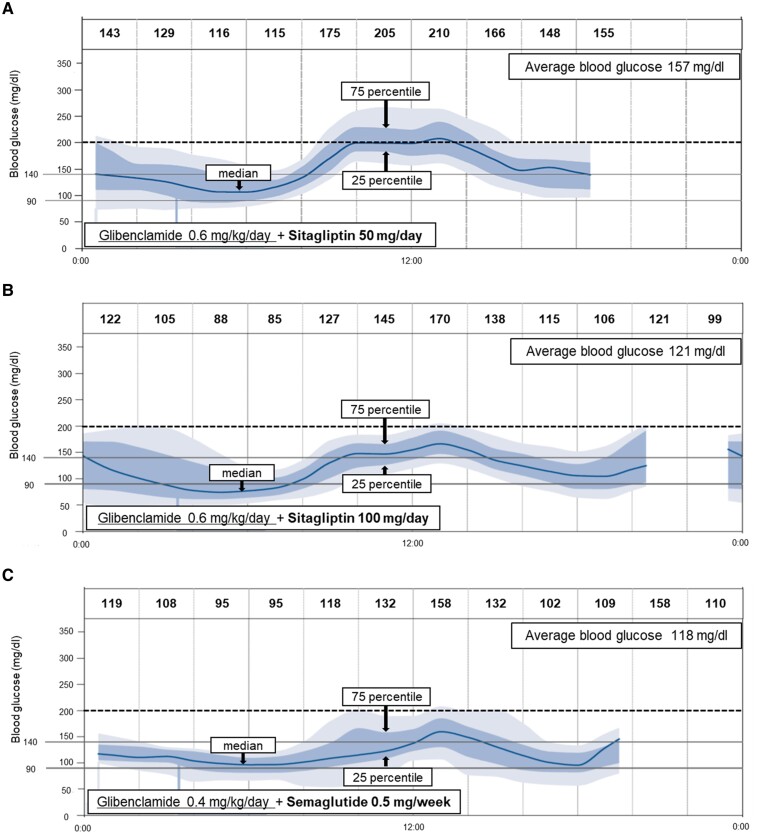
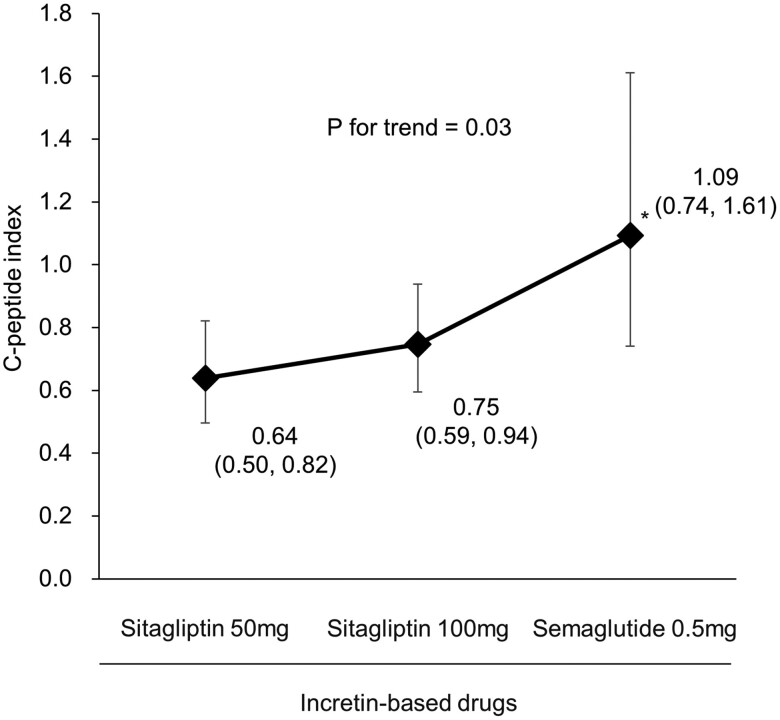
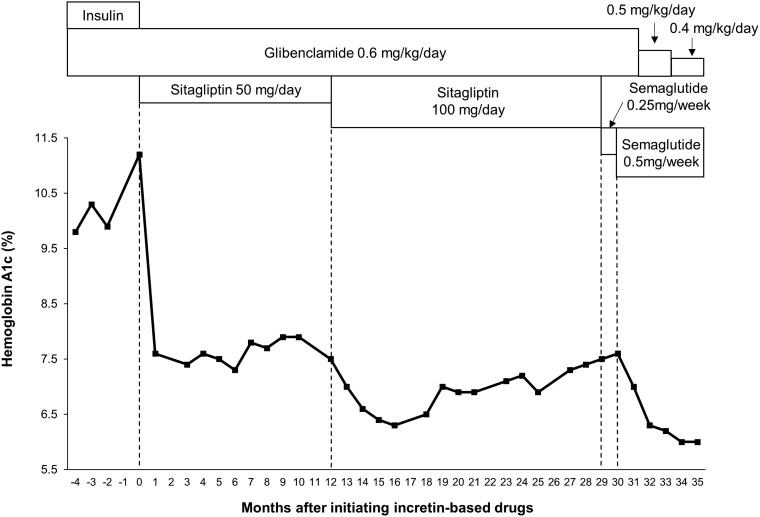
Permanent neonatal diabetes mellitus (PNDM) is a genetic disorder, characterized by a decrease in endogenous insulin secretion. Therefore, exogenous insulin supplementation plays a central role in controlling glycemia. Although adding a sulfonylurea can help to discontinue insulin, discontinuation is sometimes difficult when the sulfonylurea is administered at older ages. A 24-year-old woman with longstanding PNDM who had poor glycemic control using insulin (47 U/day) and high-dose glibenclamide (0.6 mg/kg/day), had successfully discontinued insulin after initiating the dipeptidyl peptidase-4 inhibitor sitagliptin (50 mg/day). Additionally, hemoglobin A1c levels decreased by 4.8%. Double dosing of sitagliptin and subsequent switching to the glucagon-like peptide-1 receptor agonist semaglutide (0.25 mg/week followed by 0.5 mg/week) further decreased hemoglobin A1c values, with graded improvements in endogenous insulin secretion. There were no episodes of hypoglycemia during which glibenclamide was titrated down from 0.6 to 0.4 mg/kg/day. Intra- and inter-day glucose variability as assessed by continuous glucose monitoring was also improved. In patients with PNDM, administration and dose escalation of incretin-based drugs, in addition to a high-dose sulfonylurea, could be a useful treatment strategy. This strategy may be helpful for discontinuing insulin, downtitrating sulfonylureas, and subsequent achievement of better glycemic control regarding long-term stability and short-term variability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


