Xuan Wang, Anna M Plantinga, Xin Xiong, Sara J Cromer, Clara-Lea Bonzel, Vidul Panickan, Rui Duan, Jue Hou, Tianxi Cai
{"title":"比较胰岛素与胰高血糖素样肽-1 受体激动剂、二肽基肽酶-4 抑制剂和钠-葡萄糖客转运体 2 抑制剂对 2 型糖尿病患者 5 年心衰发病风险的影响:利用保险索赔进行的真实世界证据研究。","authors":"Xuan Wang, Anna M Plantinga, Xin Xiong, Sara J Cromer, Clara-Lea Bonzel, Vidul Panickan, Rui Duan, Jue Hou, Tianxi Cai","doi":"10.2196/58137","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Type 2 diabetes mellitus (T2DM) is a common health issue, with heart failure (HF) being a common and lethal long-term complication. Although insulin is widely used for the treatment of T2DM, evidence regarding the efficacy of insulin compared to noninsulin therapies on incident HF risk is missing among randomized controlled trials. Real-world evidence on insulin's effect on long-term HF risk may supplement existing guidelines on the management of T2DM.</p><p><strong>Objective: </strong>This study aimed to compare insulin therapy against other medications on HF risk among patients with T2DM using real-world data extracted from insurance claims.</p><p><strong>Methods: </strong>A retrospective, observational study was conducted based on insurance claims data from a single health care network. The study period was from January 1, 2016, to August 11, 2021. The cohort was defined as patients having a T2DM diagnosis code. The inclusion criteria were patients who had at least 1 record of a glycated hemoglobin laboratory test result; full insurance for at least 1 year (either commercial or Medicare Part D); and received glucose-lowering therapy belonging to 1 of the following groups: insulin, glucagon-like peptide 1 receptor agonists (GLP-1 RAs), dipeptidyl peptidase-4 inhibitors (DPP-4Is), or sodium-glucose cotransporter-2 inhibitors (SGLT2Is). The main outcome was the 5-year incident HF rate. Baseline covariates, including demographic characteristics, comorbidities, and laboratory test results, were adjusted to correct for confounding.</p><p><strong>Results: </strong>After adjusting for a broad list of confounders, patients receiving insulin were found to be associated with an 11.8% (95% CI 11.0%-12.7%), 12.0% (95% CI 11.5%-12.4%), and 15.1% (95% CI 14.3%-16.0%) higher 5-year HF rate compared to those using GLP-1 RAs, DPP-4Is, and SGLT2Is, respectively. Subgroup analysis showed that insulin's effect of a higher HF rate was significant in the subgroup with high HF risk but not significant in the subgroup with low HF risk.</p><p><strong>Conclusions: </strong>This study generated real-world evidence on the association of insulin therapy with a higher 5-year HF rate compared to GLP-1 RAs, DPP-4Is, and SGLT2Is based on insurance claims data. These findings also demonstrated the value of real-world data for comparative effectiveness studies to complement established guidelines. On the other hand, the study shares the common limitations of observational studies. Even though high-dimensional confounders are adjusted, remaining confounding may exist and induce bias in the analysis.</p>","PeriodicalId":52371,"journal":{"name":"JMIR Diabetes","volume":"9 ","pages":"e58137"},"PeriodicalIF":2.6000,"publicationDate":"2024-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11520261/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparing Insulin Against Glucagon-Like Peptide-1 Receptor Agonists, Dipeptidyl Peptidase-4 Inhibitors, and Sodium-Glucose Cotransporter 2 Inhibitors on 5-Year Incident Heart Failure Risk for Patients With Type 2 Diabetes Mellitus: Real-World Evidence Study Using Insurance Claims.\",\"authors\":\"Xuan Wang, Anna M Plantinga, Xin Xiong, Sara J Cromer, Clara-Lea Bonzel, Vidul Panickan, Rui Duan, Jue Hou, Tianxi Cai\",\"doi\":\"10.2196/58137\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Type 2 diabetes mellitus (T2DM) is a common health issue, with heart failure (HF) being a common and lethal long-term complication. Although insulin is widely used for the treatment of T2DM, evidence regarding the efficacy of insulin compared to noninsulin therapies on incident HF risk is missing among randomized controlled trials. Real-world evidence on insulin's effect on long-term HF risk may supplement existing guidelines on the management of T2DM.</p><p><strong>Objective: </strong>This study aimed to compare insulin therapy against other medications on HF risk among patients with T2DM using real-world data extracted from insurance claims.</p><p><strong>Methods: </strong>A retrospective, observational study was conducted based on insurance claims data from a single health care network. The study period was from January 1, 2016, to August 11, 2021. The cohort was defined as patients having a T2DM diagnosis code. The inclusion criteria were patients who had at least 1 record of a glycated hemoglobin laboratory test result; full insurance for at least 1 year (either commercial or Medicare Part D); and received glucose-lowering therapy belonging to 1 of the following groups: insulin, glucagon-like peptide 1 receptor agonists (GLP-1 RAs), dipeptidyl peptidase-4 inhibitors (DPP-4Is), or sodium-glucose cotransporter-2 inhibitors (SGLT2Is). The main outcome was the 5-year incident HF rate. Baseline covariates, including demographic characteristics, comorbidities, and laboratory test results, were adjusted to correct for confounding.</p><p><strong>Results: </strong>After adjusting for a broad list of confounders, patients receiving insulin were found to be associated with an 11.8% (95% CI 11.0%-12.7%), 12.0% (95% CI 11.5%-12.4%), and 15.1% (95% CI 14.3%-16.0%) higher 5-year HF rate compared to those using GLP-1 RAs, DPP-4Is, and SGLT2Is, respectively. Subgroup analysis showed that insulin's effect of a higher HF rate was significant in the subgroup with high HF risk but not significant in the subgroup with low HF risk.</p><p><strong>Conclusions: </strong>This study generated real-world evidence on the association of insulin therapy with a higher 5-year HF rate compared to GLP-1 RAs, DPP-4Is, and SGLT2Is based on insurance claims data. These findings also demonstrated the value of real-world data for comparative effectiveness studies to complement established guidelines. On the other hand, the study shares the common limitations of observational studies. Even though high-dimensional confounders are adjusted, remaining confounding may exist and induce bias in the analysis.</p>\",\"PeriodicalId\":52371,\"journal\":{\"name\":\"JMIR Diabetes\",\"volume\":\"9 \",\"pages\":\"e58137\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-10-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11520261/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Diabetes\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/58137\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Diabetes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/58137","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Comparing Insulin Against Glucagon-Like Peptide-1 Receptor Agonists, Dipeptidyl Peptidase-4 Inhibitors, and Sodium-Glucose Cotransporter 2 Inhibitors on 5-Year Incident Heart Failure Risk for Patients With Type 2 Diabetes Mellitus: Real-World Evidence Study Using Insurance Claims.
Background: Type 2 diabetes mellitus (T2DM) is a common health issue, with heart failure (HF) being a common and lethal long-term complication. Although insulin is widely used for the treatment of T2DM, evidence regarding the efficacy of insulin compared to noninsulin therapies on incident HF risk is missing among randomized controlled trials. Real-world evidence on insulin's effect on long-term HF risk may supplement existing guidelines on the management of T2DM.
Objective: This study aimed to compare insulin therapy against other medications on HF risk among patients with T2DM using real-world data extracted from insurance claims.
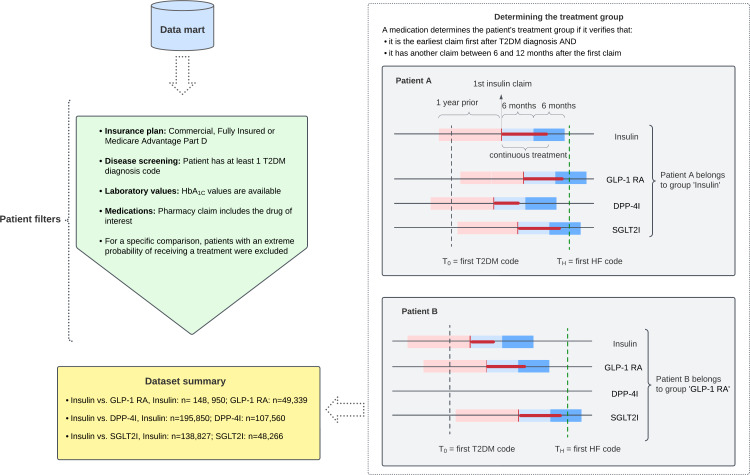
Methods: A retrospective, observational study was conducted based on insurance claims data from a single health care network. The study period was from January 1, 2016, to August 11, 2021. The cohort was defined as patients having a T2DM diagnosis code. The inclusion criteria were patients who had at least 1 record of a glycated hemoglobin laboratory test result; full insurance for at least 1 year (either commercial or Medicare Part D); and received glucose-lowering therapy belonging to 1 of the following groups: insulin, glucagon-like peptide 1 receptor agonists (GLP-1 RAs), dipeptidyl peptidase-4 inhibitors (DPP-4Is), or sodium-glucose cotransporter-2 inhibitors (SGLT2Is). The main outcome was the 5-year incident HF rate. Baseline covariates, including demographic characteristics, comorbidities, and laboratory test results, were adjusted to correct for confounding.
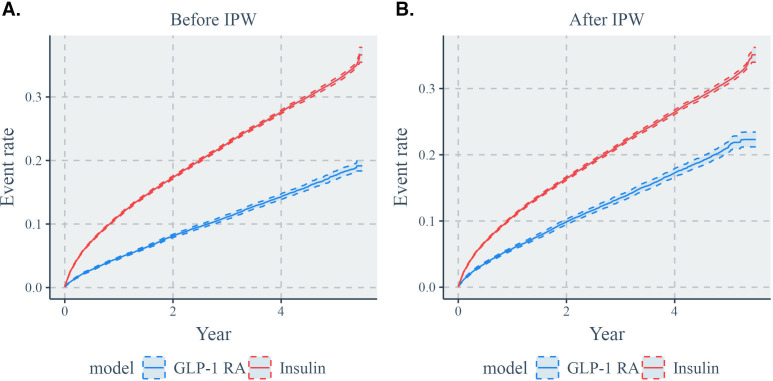
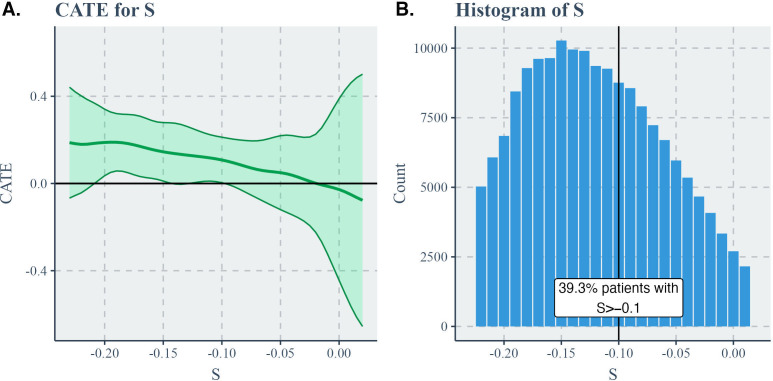
Results: After adjusting for a broad list of confounders, patients receiving insulin were found to be associated with an 11.8% (95% CI 11.0%-12.7%), 12.0% (95% CI 11.5%-12.4%), and 15.1% (95% CI 14.3%-16.0%) higher 5-year HF rate compared to those using GLP-1 RAs, DPP-4Is, and SGLT2Is, respectively. Subgroup analysis showed that insulin's effect of a higher HF rate was significant in the subgroup with high HF risk but not significant in the subgroup with low HF risk.
Conclusions: This study generated real-world evidence on the association of insulin therapy with a higher 5-year HF rate compared to GLP-1 RAs, DPP-4Is, and SGLT2Is based on insurance claims data. These findings also demonstrated the value of real-world data for comparative effectiveness studies to complement established guidelines. On the other hand, the study shares the common limitations of observational studies. Even though high-dimensional confounders are adjusted, remaining confounding may exist and induce bias in the analysis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


