Jorun Tangen, Thuy Mi Nguyen, Daniela Melichova, Lars Gunnar Klaeboe, Marianne Forsa, Kristoffer Andresen, Adrien Al Wazzan, Oyvind Lie, Fatih Kizilaslan, Kristina Haugaa, Helge Skulstad, Harald Brunvand, Thor Edvardsen
{"title":"通过超声心动图评估左心房容积,确定急性心肌梗死后不良预后风险高的患者。","authors":"Jorun Tangen, Thuy Mi Nguyen, Daniela Melichova, Lars Gunnar Klaeboe, Marianne Forsa, Kristoffer Andresen, Adrien Al Wazzan, Oyvind Lie, Fatih Kizilaslan, Kristina Haugaa, Helge Skulstad, Harald Brunvand, Thor Edvardsen","doi":"10.1186/s44156-024-00060-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The left atrial (LA) volume has been demonstrated to be an important predictor of adverse outcome in patients with various cardiac conditions, including acute myocardial infarction (AMI). However, new treatment strategies in patients with AMI have led to better patient outcomes. We hypothesised that increased LA size could still predict mortality in patients with AMI despite improved treatment strategies.</p><p><strong>Methods: </strong>We included patients with AMI in a prospective multicenter cohort study and the study patients were enrolled from 2014 to 2022. We recorded echocardiographic and clinical data during their index hospitalisation. Indexed LA volume (LAVi) was assessed in all patients and was used as a continuous variable in the univariate and multivariate Cox regression analysis. The study took place over a period of five years and median follow-up time was 3.8 years (range 3.1 to 5.0 years). The primary study outcomes were all-cause mortality and major adverse cardiac events (MACE). MACE was defined as hospital readmission due to myocardial infarction, cardiac arrest, stroke, heart failure, or onset of new atrial fibrillation.</p><p><strong>Results: </strong>We included 487 patients (69 ± 12 years old, 26% female) with AMI. During the follow-up period all-cause mortality was 50 (10.3%) and patients who reached the primary outcomes were 153 (31.4%). The deceased patients had higher LAVi compared to survivors (40.0 ± 12.9 mL/m<sup>2</sup> vs. 29.7 ± 11.2 mL/m<sup>2</sup>, p < 0.001). Factors associated with all-cause mortality and MACE were age, year of enrollment, left ventricular (LV) ejection fraction, LV global longitudinal strain (GLS), LV filling pressure, moderate or severe mitral regurgitation and LAVi. GLS and EF were segregated into two distinct models due to their moderately high correlation (r = 0.57, p < 0.001). LAVi remained as an independent echocardiographic predictor of primary outcomes after adjusting for the covariates above in two separates multivariable Cox regression models (hazard ratio 1.02/1.02 mL/m<sup>2</sup> [95% CI 1.01-1.03/1.01-1.03], p = 0.006/0.003).</p><p><strong>Conclusions: </strong>Our study demonstrated that LA dilatation is an independent echocardiographic predictor of mortality and MACE in patients with AMI despite improved treatment strategies. This finding highlights the potential of using LAVi as a marker for prognostication in these patients.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"11 1","pages":"24"},"PeriodicalIF":2.4000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11492485/pdf/","citationCount":"0","resultStr":"{\"title\":\"Left atrial volume assessed by echocardiography identifies patients with high risk of adverse outcome after acute myocardial infarction.\",\"authors\":\"Jorun Tangen, Thuy Mi Nguyen, Daniela Melichova, Lars Gunnar Klaeboe, Marianne Forsa, Kristoffer Andresen, Adrien Al Wazzan, Oyvind Lie, Fatih Kizilaslan, Kristina Haugaa, Helge Skulstad, Harald Brunvand, Thor Edvardsen\",\"doi\":\"10.1186/s44156-024-00060-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The left atrial (LA) volume has been demonstrated to be an important predictor of adverse outcome in patients with various cardiac conditions, including acute myocardial infarction (AMI). However, new treatment strategies in patients with AMI have led to better patient outcomes. We hypothesised that increased LA size could still predict mortality in patients with AMI despite improved treatment strategies.</p><p><strong>Methods: </strong>We included patients with AMI in a prospective multicenter cohort study and the study patients were enrolled from 2014 to 2022. We recorded echocardiographic and clinical data during their index hospitalisation. Indexed LA volume (LAVi) was assessed in all patients and was used as a continuous variable in the univariate and multivariate Cox regression analysis. The study took place over a period of five years and median follow-up time was 3.8 years (range 3.1 to 5.0 years). The primary study outcomes were all-cause mortality and major adverse cardiac events (MACE). MACE was defined as hospital readmission due to myocardial infarction, cardiac arrest, stroke, heart failure, or onset of new atrial fibrillation.</p><p><strong>Results: </strong>We included 487 patients (69 ± 12 years old, 26% female) with AMI. During the follow-up period all-cause mortality was 50 (10.3%) and patients who reached the primary outcomes were 153 (31.4%). The deceased patients had higher LAVi compared to survivors (40.0 ± 12.9 mL/m<sup>2</sup> vs. 29.7 ± 11.2 mL/m<sup>2</sup>, p < 0.001). Factors associated with all-cause mortality and MACE were age, year of enrollment, left ventricular (LV) ejection fraction, LV global longitudinal strain (GLS), LV filling pressure, moderate or severe mitral regurgitation and LAVi. GLS and EF were segregated into two distinct models due to their moderately high correlation (r = 0.57, p < 0.001). LAVi remained as an independent echocardiographic predictor of primary outcomes after adjusting for the covariates above in two separates multivariable Cox regression models (hazard ratio 1.02/1.02 mL/m<sup>2</sup> [95% CI 1.01-1.03/1.01-1.03], p = 0.006/0.003).</p><p><strong>Conclusions: </strong>Our study demonstrated that LA dilatation is an independent echocardiographic predictor of mortality and MACE in patients with AMI despite improved treatment strategies. This finding highlights the potential of using LAVi as a marker for prognostication in these patients.</p>\",\"PeriodicalId\":45749,\"journal\":{\"name\":\"Echo Research and Practice\",\"volume\":\"11 1\",\"pages\":\"24\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-10-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11492485/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Echo Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44156-024-00060-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-024-00060-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:左心房(LA)容积已被证实是预测包括急性心肌梗死(AMI)在内的各种心脏病患者不良预后的重要指标。然而,针对急性心肌梗塞患者的新治疗策略已为患者带来了更好的预后。我们假设,尽管治疗策略有所改进,但 LA 的增大仍能预测 AMI 患者的死亡率:我们在一项前瞻性多中心队列研究中纳入了急性心肌梗死患者,研究患者的入组时间为 2014 年至 2022 年。我们记录了患者住院期间的超声心动图和临床数据。我们评估了所有患者的指数 LA 容积(LAVi),并将其作为单变量和多变量 Cox 回归分析中的连续变量。研究历时五年,中位随访时间为 3.8 年(3.1 至 5.0 年)。主要研究结果为全因死亡率和主要心脏不良事件(MACE)。MACE的定义是因心肌梗死、心脏骤停、中风、心力衰竭或新发心房颤动而再次入院:我们纳入了 487 名急性心肌梗死患者(69 ± 12 岁,26% 为女性)。随访期间,全因死亡率为 50 例(10.3%),达到主要结果的患者为 153 例(31.4%)。与幸存者相比,死亡患者的 LAVi 较高(40.0 ± 12.9 mL/m2 vs. 29.7 ± 11.2 mL/m2,P 2 [95% CI 1.01-1.03/1.01-1.03],P = 0.006/0.003):我们的研究表明,尽管治疗策略有所改善,但LA扩张仍是预测AMI患者死亡率和MACE的独立超声心动图指标。这一发现凸显了将 LAVi 作为这些患者预后标志物的潜力。
Left atrial volume assessed by echocardiography identifies patients with high risk of adverse outcome after acute myocardial infarction.
Background: The left atrial (LA) volume has been demonstrated to be an important predictor of adverse outcome in patients with various cardiac conditions, including acute myocardial infarction (AMI). However, new treatment strategies in patients with AMI have led to better patient outcomes. We hypothesised that increased LA size could still predict mortality in patients with AMI despite improved treatment strategies.
Methods: We included patients with AMI in a prospective multicenter cohort study and the study patients were enrolled from 2014 to 2022. We recorded echocardiographic and clinical data during their index hospitalisation. Indexed LA volume (LAVi) was assessed in all patients and was used as a continuous variable in the univariate and multivariate Cox regression analysis. The study took place over a period of five years and median follow-up time was 3.8 years (range 3.1 to 5.0 years). The primary study outcomes were all-cause mortality and major adverse cardiac events (MACE). MACE was defined as hospital readmission due to myocardial infarction, cardiac arrest, stroke, heart failure, or onset of new atrial fibrillation.
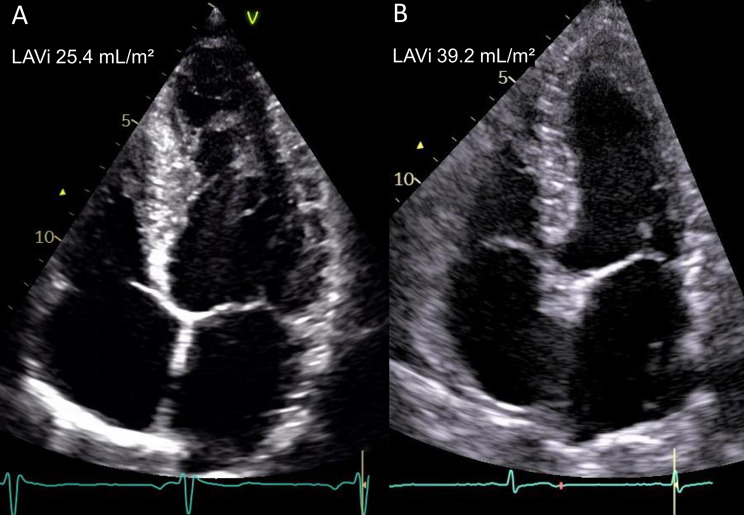
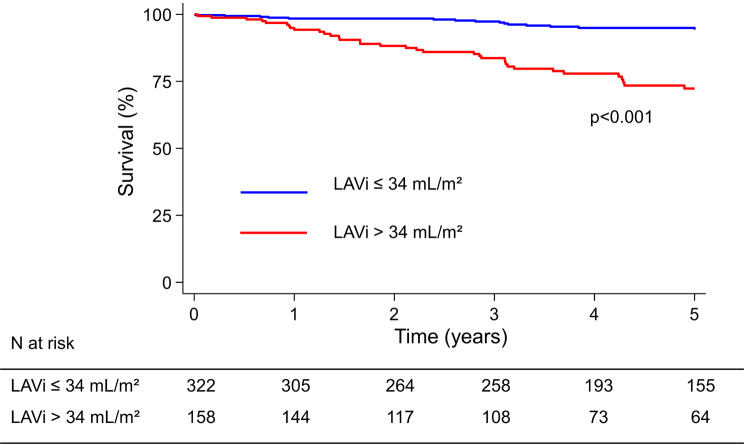
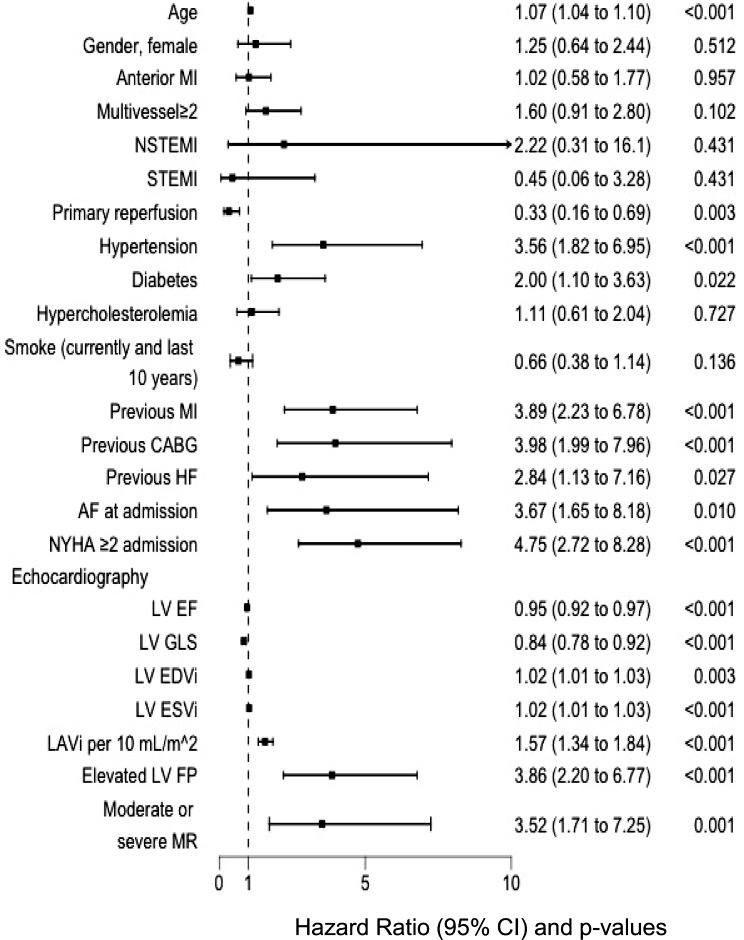
Results: We included 487 patients (69 ± 12 years old, 26% female) with AMI. During the follow-up period all-cause mortality was 50 (10.3%) and patients who reached the primary outcomes were 153 (31.4%). The deceased patients had higher LAVi compared to survivors (40.0 ± 12.9 mL/m2 vs. 29.7 ± 11.2 mL/m2, p < 0.001). Factors associated with all-cause mortality and MACE were age, year of enrollment, left ventricular (LV) ejection fraction, LV global longitudinal strain (GLS), LV filling pressure, moderate or severe mitral regurgitation and LAVi. GLS and EF were segregated into two distinct models due to their moderately high correlation (r = 0.57, p < 0.001). LAVi remained as an independent echocardiographic predictor of primary outcomes after adjusting for the covariates above in two separates multivariable Cox regression models (hazard ratio 1.02/1.02 mL/m2 [95% CI 1.01-1.03/1.01-1.03], p = 0.006/0.003).
Conclusions: Our study demonstrated that LA dilatation is an independent echocardiographic predictor of mortality and MACE in patients with AMI despite improved treatment strategies. This finding highlights the potential of using LAVi as a marker for prognostication in these patients.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


