{"title":"闭环医嘱执行系统对一家三级医院安全用药的影响:一项准实验研究。","authors":"Xuwen Yin, Haiyan Song, Jieyu Lu, Jing Yang, Rong Wang, Zheng Lin, Shudi Jiang, Hui Yuan, Xumei Wang, Dongmei Xu, Chunhong Gao, Yuan Zhou, Jiayi Xu, Chen Chen, Chenyu Gu, Qingqing Diao, Fang Li, Zejuan Gu","doi":"10.1177/20420986241288421","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Closed-loop electronic medication management systems are effective measures for preventing medication errors (MEs). However, there is limited evidence supporting this, and few studies have evaluated the long-term effects of these systems on safe medication.</p><p><strong>Objective: </strong>To evaluate the long-term effects of implementing a closed-loop medication order executive system on the safe clinical use of medications.</p><p><strong>Design: </strong>A quasi-experimental design.</p><p><strong>Method: </strong>Data from 2017 to 2023 were extracted and retrospectively analyzed. The primary outcome indicator was the ME rate. Secondary outcome indicators were the accuracy of order verification and patient identification and the implementation rate of fresh medicine dispensing. The autoregressive integrated moving average (ARIMA) model in time-series analysis was used to evaluate the level and trend changes in ME rates using SPSS 25.0 before and after system implementation. Root cause analysis and descriptive statistics were used to assess changes in types, stages, and causes of ME rates. The independent samples <i>t</i>-test was used to analyze secondary outcomes.</p><p><strong>Results: </strong>Overall, 295 MEs were reported with a mean of 0.26 ± 0.26 ME rates per month during 2017-2023. The ARIMA model showed a decrease in the average level of ME rates after system implementation, with no statistically significant decrease in the long term, and a significant drop in the ME rate in the short and medium term (<i>p</i> < 0.01). Nurses' administration accounted for more than 60% of errors post-implementation, and lack of communication was a prominent factor. The accuracy of order verification and patient identification and the implementation rate of fresh medicine dispensing all increased after implementation.</p><p><strong>Conclusion: </strong>Adopting a closed-loop executive system is beneficial for ensuring patient medication safety, but a single integrated system does not completely eliminate MEs. Optimizing system functionalities and applying structured handoff tools are recommended to meet clinical needs and enhance system usability.</p>","PeriodicalId":23012,"journal":{"name":"Therapeutic Advances in Drug Safety","volume":"15 ","pages":"20420986241288421"},"PeriodicalIF":3.4000,"publicationDate":"2024-10-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11472417/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of a closed-loop medication order executive system on safe medication administration at a tertiary hospital: a quasi-experimental study.\",\"authors\":\"Xuwen Yin, Haiyan Song, Jieyu Lu, Jing Yang, Rong Wang, Zheng Lin, Shudi Jiang, Hui Yuan, Xumei Wang, Dongmei Xu, Chunhong Gao, Yuan Zhou, Jiayi Xu, Chen Chen, Chenyu Gu, Qingqing Diao, Fang Li, Zejuan Gu\",\"doi\":\"10.1177/20420986241288421\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Closed-loop electronic medication management systems are effective measures for preventing medication errors (MEs). However, there is limited evidence supporting this, and few studies have evaluated the long-term effects of these systems on safe medication.</p><p><strong>Objective: </strong>To evaluate the long-term effects of implementing a closed-loop medication order executive system on the safe clinical use of medications.</p><p><strong>Design: </strong>A quasi-experimental design.</p><p><strong>Method: </strong>Data from 2017 to 2023 were extracted and retrospectively analyzed. The primary outcome indicator was the ME rate. Secondary outcome indicators were the accuracy of order verification and patient identification and the implementation rate of fresh medicine dispensing. The autoregressive integrated moving average (ARIMA) model in time-series analysis was used to evaluate the level and trend changes in ME rates using SPSS 25.0 before and after system implementation. Root cause analysis and descriptive statistics were used to assess changes in types, stages, and causes of ME rates. The independent samples <i>t</i>-test was used to analyze secondary outcomes.</p><p><strong>Results: </strong>Overall, 295 MEs were reported with a mean of 0.26 ± 0.26 ME rates per month during 2017-2023. The ARIMA model showed a decrease in the average level of ME rates after system implementation, with no statistically significant decrease in the long term, and a significant drop in the ME rate in the short and medium term (<i>p</i> < 0.01). Nurses' administration accounted for more than 60% of errors post-implementation, and lack of communication was a prominent factor. The accuracy of order verification and patient identification and the implementation rate of fresh medicine dispensing all increased after implementation.</p><p><strong>Conclusion: </strong>Adopting a closed-loop executive system is beneficial for ensuring patient medication safety, but a single integrated system does not completely eliminate MEs. Optimizing system functionalities and applying structured handoff tools are recommended to meet clinical needs and enhance system usability.</p>\",\"PeriodicalId\":23012,\"journal\":{\"name\":\"Therapeutic Advances in Drug Safety\",\"volume\":\"15 \",\"pages\":\"20420986241288421\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-10-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11472417/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20420986241288421\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420986241288421","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
摘要
背景:闭环电子用药管理系统是预防用药错误(ME)的有效措施。然而,支持这一观点的证据有限,很少有研究评估了这些系统对安全用药的长期影响:目的:评估实施闭环医嘱执行系统对临床安全用药的长期影响:准实验设计:提取2017年至2023年的数据并进行回顾性分析。主要结果指标为ME率。次要结果指标为医嘱核对和患者身份识别准确率以及新鲜药品发放执行率。使用 SPSS 25.0 进行时间序列分析时,采用了自回归综合移动平均(ARIMA)模型来评估系统实施前后 ME 率的水平和趋势变化。使用根本原因分析和描述性统计来评估 ME 发生率的类型、阶段和原因的变化。采用独立样本 t 检验分析次要结果:总体而言,2017-2023年期间共报告了295例ME,平均每月ME率为0.26±0.26。ARIMA模型显示,系统实施后,ME率平均水平有所下降,长期下降幅度无统计学意义,中短期ME率显著下降(p 结论:系统实施后,ME率平均水平有所下降,长期下降幅度无统计学意义,中短期ME率显著下降(p 结论:系统实施后,ME率平均水平有所下降,长期下降幅度无统计学意义,中短期ME率显著下降:采用闭环执行系统有利于确保患者的用药安全,但单一的综合系统并不能完全消除 ME。建议优化系统功能并应用结构化交接工具,以满足临床需求并提高系统可用性。
Effect of a closed-loop medication order executive system on safe medication administration at a tertiary hospital: a quasi-experimental study.
Background: Closed-loop electronic medication management systems are effective measures for preventing medication errors (MEs). However, there is limited evidence supporting this, and few studies have evaluated the long-term effects of these systems on safe medication.
Objective: To evaluate the long-term effects of implementing a closed-loop medication order executive system on the safe clinical use of medications.
Design: A quasi-experimental design.
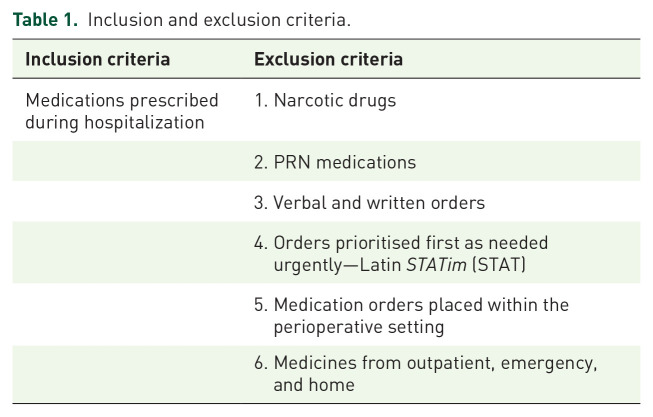
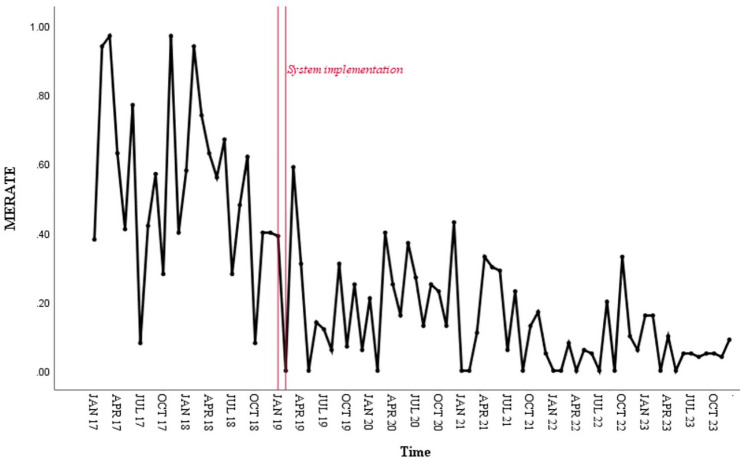
Method: Data from 2017 to 2023 were extracted and retrospectively analyzed. The primary outcome indicator was the ME rate. Secondary outcome indicators were the accuracy of order verification and patient identification and the implementation rate of fresh medicine dispensing. The autoregressive integrated moving average (ARIMA) model in time-series analysis was used to evaluate the level and trend changes in ME rates using SPSS 25.0 before and after system implementation. Root cause analysis and descriptive statistics were used to assess changes in types, stages, and causes of ME rates. The independent samples t-test was used to analyze secondary outcomes.
Results: Overall, 295 MEs were reported with a mean of 0.26 ± 0.26 ME rates per month during 2017-2023. The ARIMA model showed a decrease in the average level of ME rates after system implementation, with no statistically significant decrease in the long term, and a significant drop in the ME rate in the short and medium term (p < 0.01). Nurses' administration accounted for more than 60% of errors post-implementation, and lack of communication was a prominent factor. The accuracy of order verification and patient identification and the implementation rate of fresh medicine dispensing all increased after implementation.
Conclusion: Adopting a closed-loop executive system is beneficial for ensuring patient medication safety, but a single integrated system does not completely eliminate MEs. Optimizing system functionalities and applying structured handoff tools are recommended to meet clinical needs and enhance system usability.
期刊介绍:
Therapeutic Advances in Drug Safety delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies pertaining to the safe use of drugs in patients.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in drug safety, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest on research across all areas of drug safety, including therapeutic drug monitoring, pharmacoepidemiology, adverse drug reactions, drug interactions, pharmacokinetics, pharmacovigilance, medication/prescribing errors, risk management, ethics and regulation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


