{"title":"男性黄褐斑:一个鲜为人知的实体。","authors":"Tim Aung, Rowland Noakes","doi":"10.5694/mja2.52478","DOIUrl":null,"url":null,"abstract":"<p>An otherwise healthy man of Southeast-Asian descent aged in his mid-30s presented with non-pruritic hyperpigmented patches involving the face for over 12 months (Figure). Clinically, the findings were consistent with melasma, characterised by brown or dark brown hyperpigmented patches with demarcated or ill-defined borders, involving the face (zygoma and cheeks) bilaterally. There was no history or clinical features suggestive of diagnoses such as post-inflammatory hyperpigmentation, drug-induced pigmentation or photosensitivity, or actinic lichen planus.</p><p>Melasma is a common acquired hyperpigmentary condition, described mostly in women of Asian, Middle Eastern or Latin American descent aged 30–50 years.<span><sup>1</sup></span> Melasma in men is less well recognised,<span><sup>2</sup></span> with a reported sex ratio of 1:9 (male:female).<span><sup>3</sup></span> The precise aetiopathogenesis of melasma is incompletely understood. However, there are risk factors related to melasma development, such as sunlight exposure, genetic predisposition, hormonal exposure (contraceptive use and pregnancy), photosensitive medications and cosmetics use, and, rarely, thyroid disorder.<span><sup>2-5</sup></span> Melasma can be diagnosed clinically based on distribution and characteristics of pigmentation and skin type or ethnicity; biopsy is rarely required.</p><p>Management includes sun protection with the use of a wide-brim hat and sunscreen (with a sun protection factor of 30 or over), and avoidance of risk factors such as phototoxic drugs, cosmetics, and hormonal contraception (in women). The triple combined topical therapy (hydroquinone 4–5% with tretinoin 0.05–0.1% and low potency corticosteroid), daily for three months, is usually the first line treatment of choice.<span><sup>1-3</sup></span> Adjunct oral tranexamic acid may be considered for extensive lesions, dermal involvement, or for patients refractory to topical therapy, although there are no established studies in men.<span><sup>2</sup></span> There are also advanced treatment options, such as chemical peeling, microneedling, and light and laser-based therapies, with unpredictable or mixed results.<span><sup>1, 3</sup></span></p><p>Open access publishing facilitated by the University of Queensland, as part of the Wiley – the University of Queensland agreement via the Council of Australian University Librarians.</p><p>No relevant disclosures.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 9","pages":"468"},"PeriodicalIF":6.7000,"publicationDate":"2024-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52478","citationCount":"0","resultStr":"{\"title\":\"Melasma in the male: a less well recognised entity\",\"authors\":\"Tim Aung, Rowland Noakes\",\"doi\":\"10.5694/mja2.52478\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>An otherwise healthy man of Southeast-Asian descent aged in his mid-30s presented with non-pruritic hyperpigmented patches involving the face for over 12 months (Figure). Clinically, the findings were consistent with melasma, characterised by brown or dark brown hyperpigmented patches with demarcated or ill-defined borders, involving the face (zygoma and cheeks) bilaterally. There was no history or clinical features suggestive of diagnoses such as post-inflammatory hyperpigmentation, drug-induced pigmentation or photosensitivity, or actinic lichen planus.</p><p>Melasma is a common acquired hyperpigmentary condition, described mostly in women of Asian, Middle Eastern or Latin American descent aged 30–50 years.<span><sup>1</sup></span> Melasma in men is less well recognised,<span><sup>2</sup></span> with a reported sex ratio of 1:9 (male:female).<span><sup>3</sup></span> The precise aetiopathogenesis of melasma is incompletely understood. However, there are risk factors related to melasma development, such as sunlight exposure, genetic predisposition, hormonal exposure (contraceptive use and pregnancy), photosensitive medications and cosmetics use, and, rarely, thyroid disorder.<span><sup>2-5</sup></span> Melasma can be diagnosed clinically based on distribution and characteristics of pigmentation and skin type or ethnicity; biopsy is rarely required.</p><p>Management includes sun protection with the use of a wide-brim hat and sunscreen (with a sun protection factor of 30 or over), and avoidance of risk factors such as phototoxic drugs, cosmetics, and hormonal contraception (in women). The triple combined topical therapy (hydroquinone 4–5% with tretinoin 0.05–0.1% and low potency corticosteroid), daily for three months, is usually the first line treatment of choice.<span><sup>1-3</sup></span> Adjunct oral tranexamic acid may be considered for extensive lesions, dermal involvement, or for patients refractory to topical therapy, although there are no established studies in men.<span><sup>2</sup></span> There are also advanced treatment options, such as chemical peeling, microneedling, and light and laser-based therapies, with unpredictable or mixed results.<span><sup>1, 3</sup></span></p><p>Open access publishing facilitated by the University of Queensland, as part of the Wiley – the University of Queensland agreement via the Council of Australian University Librarians.</p><p>No relevant disclosures.</p>\",\"PeriodicalId\":18214,\"journal\":{\"name\":\"Medical Journal of Australia\",\"volume\":\"221 9\",\"pages\":\"468\"},\"PeriodicalIF\":6.7000,\"publicationDate\":\"2024-10-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52478\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Journal of Australia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52478\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52478","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
一名 30 多岁、身体健康的东南亚裔男子,面部出现非瘙痒性色素沉着斑块超过 12 个月(如图)。临床表现与黄褐斑一致,表现为棕色或深棕色色素沉着斑块,边界分明或不清,累及双侧面部(颧骨和脸颊)。黄褐斑是一种常见的后天性色素沉着病,多见于 30-50 岁的亚洲、中东或拉丁美洲裔女性1 。不过,黄褐斑的发生与一些风险因素有关,如日光照射、遗传倾向、激素接触(使用避孕药和怀孕)、光敏性药物和化妆品的使用,以及罕见的甲状腺疾病。黄褐斑可根据色素沉着的分布和特征以及皮肤类型或种族进行临床诊断;很少需要活组织检查。管理方法包括使用宽边帽和防晒霜(防晒系数 30 或以上)进行防晒,避免光毒性药物、化妆品和激素避孕(女性)等危险因素。三联局部疗法(氢醌 4-5%,曲安奈德 0.05-0.1% 和低效皮质类固醇)通常是首选的一线治疗方法,每天使用,连续使用三个月。1-3 如果皮损范围广、真皮受累或局部疗法难治,可考虑辅助口服氨甲环酸,但目前还没有针对男性的成熟研究。此外,还有一些先进的治疗方法,如化学换肤、微针疗法、光疗和激光疗法,但效果难以预测或好坏参半。1, 3昆士兰大学通过澳大利亚大学图书馆员理事会(Council of Australian University Librarians)与威利公司(Wiley)签订协议,为开放式出版提供便利。
Melasma in the male: a less well recognised entity
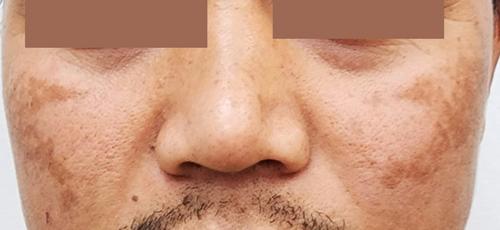
An otherwise healthy man of Southeast-Asian descent aged in his mid-30s presented with non-pruritic hyperpigmented patches involving the face for over 12 months (Figure). Clinically, the findings were consistent with melasma, characterised by brown or dark brown hyperpigmented patches with demarcated or ill-defined borders, involving the face (zygoma and cheeks) bilaterally. There was no history or clinical features suggestive of diagnoses such as post-inflammatory hyperpigmentation, drug-induced pigmentation or photosensitivity, or actinic lichen planus.
Melasma is a common acquired hyperpigmentary condition, described mostly in women of Asian, Middle Eastern or Latin American descent aged 30–50 years.1 Melasma in men is less well recognised,2 with a reported sex ratio of 1:9 (male:female).3 The precise aetiopathogenesis of melasma is incompletely understood. However, there are risk factors related to melasma development, such as sunlight exposure, genetic predisposition, hormonal exposure (contraceptive use and pregnancy), photosensitive medications and cosmetics use, and, rarely, thyroid disorder.2-5 Melasma can be diagnosed clinically based on distribution and characteristics of pigmentation and skin type or ethnicity; biopsy is rarely required.
Management includes sun protection with the use of a wide-brim hat and sunscreen (with a sun protection factor of 30 or over), and avoidance of risk factors such as phototoxic drugs, cosmetics, and hormonal contraception (in women). The triple combined topical therapy (hydroquinone 4–5% with tretinoin 0.05–0.1% and low potency corticosteroid), daily for three months, is usually the first line treatment of choice.1-3 Adjunct oral tranexamic acid may be considered for extensive lesions, dermal involvement, or for patients refractory to topical therapy, although there are no established studies in men.2 There are also advanced treatment options, such as chemical peeling, microneedling, and light and laser-based therapies, with unpredictable or mixed results.1, 3
Open access publishing facilitated by the University of Queensland, as part of the Wiley – the University of Queensland agreement via the Council of Australian University Librarians.
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


