{"title":"外阴白肌瘤伴有术后急性谵妄。","authors":"Manas Ranjan Behera, Aditya Pati, Shabnam K, Sweta Singh","doi":"10.5114/pm.2024.141094","DOIUrl":null,"url":null,"abstract":"<p><p>Leiomyomas are benign, well-circumscribed mesenchymal tumours. While uterine leiomyomas are common, vulval leiomyomas are rare. We report the challenging case of vulval leiomyoma in a multiparous woman, who also developed acute postoperative delirium. A 41-year-old multiparous woman presented with a mass in the perineum of one year duration and discomfort in a sitting position since a month ago. Her menstrual history, family history, and personal history were unremarkable. On examination of the vulva, there was a firm mass of size 10 x 8 cm on the left side, involving the labium majus and minus, which was distorting the introitus. The uterus and ovaries were normal. Preoperative ultrasound was suggestive of a vulval solid lobulated lesion, probably leiomyoma. Excision of the mass was performed. The patient developed postoperative delirium at 3 hours and was treated with an injection of haloperidol, antibiotics, and electrolyte correction. She recovered well and was discharged on the sixth postoperative day. Histopathology confirmed leiomyoma of the vulval mass, with areas of cystic degeneration. At 6-month follow-up the patient was asymptomatic and had no recurrence. To conclude, vulval leiomyoma is rare and treated by excision. The occurrence of postoperative delirium adds to the surgical morbidity, and gynaecologists should be aware of these conditions for optimal outcomes.</p>","PeriodicalId":55643,"journal":{"name":"Przeglad Menopauzalny","volume":"23 2","pages":"113-116"},"PeriodicalIF":1.7000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11462146/pdf/","citationCount":"0","resultStr":"{\"title\":\"Vulval leiomyoma with acute postoperative delirium.\",\"authors\":\"Manas Ranjan Behera, Aditya Pati, Shabnam K, Sweta Singh\",\"doi\":\"10.5114/pm.2024.141094\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Leiomyomas are benign, well-circumscribed mesenchymal tumours. While uterine leiomyomas are common, vulval leiomyomas are rare. We report the challenging case of vulval leiomyoma in a multiparous woman, who also developed acute postoperative delirium. A 41-year-old multiparous woman presented with a mass in the perineum of one year duration and discomfort in a sitting position since a month ago. Her menstrual history, family history, and personal history were unremarkable. On examination of the vulva, there was a firm mass of size 10 x 8 cm on the left side, involving the labium majus and minus, which was distorting the introitus. The uterus and ovaries were normal. Preoperative ultrasound was suggestive of a vulval solid lobulated lesion, probably leiomyoma. Excision of the mass was performed. The patient developed postoperative delirium at 3 hours and was treated with an injection of haloperidol, antibiotics, and electrolyte correction. She recovered well and was discharged on the sixth postoperative day. Histopathology confirmed leiomyoma of the vulval mass, with areas of cystic degeneration. At 6-month follow-up the patient was asymptomatic and had no recurrence. To conclude, vulval leiomyoma is rare and treated by excision. The occurrence of postoperative delirium adds to the surgical morbidity, and gynaecologists should be aware of these conditions for optimal outcomes.</p>\",\"PeriodicalId\":55643,\"journal\":{\"name\":\"Przeglad Menopauzalny\",\"volume\":\"23 2\",\"pages\":\"113-116\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11462146/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Przeglad Menopauzalny\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5114/pm.2024.141094\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Przeglad Menopauzalny","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/pm.2024.141094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
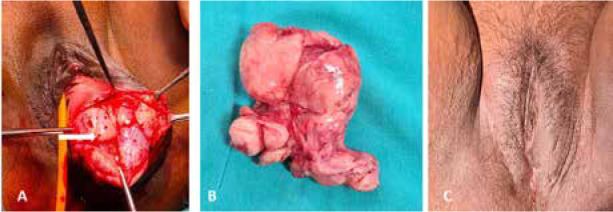
子宫纵隔肌瘤是一种良性、圆形间质肿瘤。子宫纵膈肌瘤很常见,但外阴纵膈肌瘤却很罕见。我们报告了一例具有挑战性的多产妇女外阴白肌瘤病例,该患者术后还出现了急性谵妄。一名 41 岁的多产妇因会阴部肿块就诊,病程一年,一个月前开始出现坐姿不适。她的月经史、家族史和个人史均无异常。外阴检查发现,左侧有一个 10 x 8 厘米大小的坚实肿块,累及大阴唇和小阴唇,使阴道口变形。子宫和卵巢正常。术前超声检查提示外阴实性分叶状病变,可能是子宫肌瘤。手术切除了肿块。患者术后3小时出现谵妄,接受了氟哌啶醇注射、抗生素和电解质纠正治疗。她恢复良好,并于术后第六天出院。组织病理学证实外阴肿块为子宫肌瘤,有囊性变性区域。随访6个月,患者无任何症状,也没有复发。总之,外阴白肌瘤很罕见,治疗方法是切除。术后谵妄的发生增加了手术的发病率,妇科医生应注意这些情况,以获得最佳治疗效果。
Vulval leiomyoma with acute postoperative delirium.
Leiomyomas are benign, well-circumscribed mesenchymal tumours. While uterine leiomyomas are common, vulval leiomyomas are rare. We report the challenging case of vulval leiomyoma in a multiparous woman, who also developed acute postoperative delirium. A 41-year-old multiparous woman presented with a mass in the perineum of one year duration and discomfort in a sitting position since a month ago. Her menstrual history, family history, and personal history were unremarkable. On examination of the vulva, there was a firm mass of size 10 x 8 cm on the left side, involving the labium majus and minus, which was distorting the introitus. The uterus and ovaries were normal. Preoperative ultrasound was suggestive of a vulval solid lobulated lesion, probably leiomyoma. Excision of the mass was performed. The patient developed postoperative delirium at 3 hours and was treated with an injection of haloperidol, antibiotics, and electrolyte correction. She recovered well and was discharged on the sixth postoperative day. Histopathology confirmed leiomyoma of the vulval mass, with areas of cystic degeneration. At 6-month follow-up the patient was asymptomatic and had no recurrence. To conclude, vulval leiomyoma is rare and treated by excision. The occurrence of postoperative delirium adds to the surgical morbidity, and gynaecologists should be aware of these conditions for optimal outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


