Johannes Ott, Geoffroy Robin, Marlene Hager, Didier Dewailly
{"title":"功能性下丘脑闭经与多囊卵巢形态:关于一种有趣关联的叙述性综述。","authors":"Johannes Ott, Geoffroy Robin, Marlene Hager, Didier Dewailly","doi":"10.1093/humupd/dmae030","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Functional hypothalamic amenorrhoea (FHA) is responsible for 20-35% of all cases of secondary amenorrhoea and, thus, is the second most common cause of secondary amenorrhoea after polycystic ovary syndrome (PCOS). A high number of patients with FHA reveal polycystic ovarian morphology (PCOM) on ultrasound. The combination of amenorrhoea and PCOM can lead to confusion. First, amenorrhoeic women with PCOM fulfil the revised Rotterdam criteria and, thus, can easily be misdiagnosed with PCOS. Moreover, it has been claimed that some women with FHA and concomitant PCOM differ from those without PCOM in terms of endocrine regulation and metabolic traits.</p><p><strong>Objective and rationale: </strong>The main focus of this article was on studies about FHA, which differentiated between patients with or without PCOM. The aim was to estimate the prevalence of PCOM and to look if it has an impact on pathophysiologic, diagnostic and therapeutic issues as well as on long-term consequences.</p><p><strong>Search methods: </strong>Peer review original and review articles were selected from PubMed searches for this review. Searches were performed using the search terms 'polycystic AND functional hypothalamic amenorrhoea'. The reference lists of publications found were searched for relevant additional studies. The inclusion criteria for publications were: English language, patients' age ≥ 18 years, year of publication >1980, original studies, validated diagnosis of FHA, and validated diagnosis of PCOM using transvaginal ultrasound.</p><p><strong>Outcomes: </strong>The prevalence of PCOM in women with FHA varied from 41.9% to 46.7%, which is higher than in healthy non-PCOS controls. Hypothetically, the high prevalence might be due to a mixture of silent PCOM, as in the general population, and pre-existing PCOS. Several differences in metabolic and hormonal parameters were found between FHA-PCOM and FHA-non-PCOM patients. While oestrogen deficiency is common to both groups of patients, FHA-PCOM patients have a higher BMI, higher levels of anti-Müllerian hormone (AMH) and testosterone, a higher increase in LH in the course of a GnRH test, and lower sex hormone binding globulin (SHBG) levels than FHA-non-PCOM patients. The differential diagnosis between FHA-PCOM and PCOS, especially PCOS phenotype D (PCOM and oligo-/anovulation without hyperandrogenism), can be challenging. Several parameters have been suggested, which are helpful though not absolutely reliable. They include the typical causes for FHA (excessive exercise, energy deficit, and/or psychological stress), the serum levels of LH, testosterone, and SHBG, as well as the progestin challenge test. Whether FHA-PCOM has a different risk profile for long-term consequences concerning patients' metabolic and cardiovascular situation as well as their bone mass, is unclear. Concerning therapeutic aspects, there are only few data about FHA-PCOM compared to FHA-non-PCOM. To treat anovulation, the use of pulsatile GnRH treatment seems to be equally effective in both groups. Similar to FHA-non-PCOM patients, pulsatile GnRH therapy would be more efficient than exogenous gonadotropins in FHA-PCOM patients.</p><p><strong>Wider implications: </strong>Women with FHA-PCOM present a special sub-population of FHA patients. The diagnostic pitfall of FHA-PCOM should be emphasized in clinical guidelines about FHA and PCOS. The fact that almost half of the women with FHA have an ovarian follicle excess (i.e. PCOM) in face of low gonadotropin serum levels suggests that the intra-ovarian regulation of folliculogenesis is subject to individual variations, for unknown reasons, either genetic or epigenetic. Further studies are needed to investigate this hypothesis.</p><p><strong>Registration number: </strong>Not applicable.</p>","PeriodicalId":55045,"journal":{"name":"Human Reproduction Update","volume":" ","pages":"64-79"},"PeriodicalIF":16.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11696701/pdf/","citationCount":"0","resultStr":"{\"title\":\"Functional hypothalamic amenorrhoea and polycystic ovarian morphology: a narrative review about an intriguing association.\",\"authors\":\"Johannes Ott, Geoffroy Robin, Marlene Hager, Didier Dewailly\",\"doi\":\"10.1093/humupd/dmae030\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Functional hypothalamic amenorrhoea (FHA) is responsible for 20-35% of all cases of secondary amenorrhoea and, thus, is the second most common cause of secondary amenorrhoea after polycystic ovary syndrome (PCOS). A high number of patients with FHA reveal polycystic ovarian morphology (PCOM) on ultrasound. The combination of amenorrhoea and PCOM can lead to confusion. First, amenorrhoeic women with PCOM fulfil the revised Rotterdam criteria and, thus, can easily be misdiagnosed with PCOS. Moreover, it has been claimed that some women with FHA and concomitant PCOM differ from those without PCOM in terms of endocrine regulation and metabolic traits.</p><p><strong>Objective and rationale: </strong>The main focus of this article was on studies about FHA, which differentiated between patients with or without PCOM. The aim was to estimate the prevalence of PCOM and to look if it has an impact on pathophysiologic, diagnostic and therapeutic issues as well as on long-term consequences.</p><p><strong>Search methods: </strong>Peer review original and review articles were selected from PubMed searches for this review. Searches were performed using the search terms 'polycystic AND functional hypothalamic amenorrhoea'. The reference lists of publications found were searched for relevant additional studies. The inclusion criteria for publications were: English language, patients' age ≥ 18 years, year of publication >1980, original studies, validated diagnosis of FHA, and validated diagnosis of PCOM using transvaginal ultrasound.</p><p><strong>Outcomes: </strong>The prevalence of PCOM in women with FHA varied from 41.9% to 46.7%, which is higher than in healthy non-PCOS controls. Hypothetically, the high prevalence might be due to a mixture of silent PCOM, as in the general population, and pre-existing PCOS. Several differences in metabolic and hormonal parameters were found between FHA-PCOM and FHA-non-PCOM patients. While oestrogen deficiency is common to both groups of patients, FHA-PCOM patients have a higher BMI, higher levels of anti-Müllerian hormone (AMH) and testosterone, a higher increase in LH in the course of a GnRH test, and lower sex hormone binding globulin (SHBG) levels than FHA-non-PCOM patients. The differential diagnosis between FHA-PCOM and PCOS, especially PCOS phenotype D (PCOM and oligo-/anovulation without hyperandrogenism), can be challenging. Several parameters have been suggested, which are helpful though not absolutely reliable. They include the typical causes for FHA (excessive exercise, energy deficit, and/or psychological stress), the serum levels of LH, testosterone, and SHBG, as well as the progestin challenge test. Whether FHA-PCOM has a different risk profile for long-term consequences concerning patients' metabolic and cardiovascular situation as well as their bone mass, is unclear. Concerning therapeutic aspects, there are only few data about FHA-PCOM compared to FHA-non-PCOM. To treat anovulation, the use of pulsatile GnRH treatment seems to be equally effective in both groups. Similar to FHA-non-PCOM patients, pulsatile GnRH therapy would be more efficient than exogenous gonadotropins in FHA-PCOM patients.</p><p><strong>Wider implications: </strong>Women with FHA-PCOM present a special sub-population of FHA patients. The diagnostic pitfall of FHA-PCOM should be emphasized in clinical guidelines about FHA and PCOS. The fact that almost half of the women with FHA have an ovarian follicle excess (i.e. PCOM) in face of low gonadotropin serum levels suggests that the intra-ovarian regulation of folliculogenesis is subject to individual variations, for unknown reasons, either genetic or epigenetic. Further studies are needed to investigate this hypothesis.</p><p><strong>Registration number: </strong>Not applicable.</p>\",\"PeriodicalId\":55045,\"journal\":{\"name\":\"Human Reproduction Update\",\"volume\":\" \",\"pages\":\"64-79\"},\"PeriodicalIF\":16.1000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11696701/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Human Reproduction Update\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/humupd/dmae030\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human Reproduction Update","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/humupd/dmae030","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Functional hypothalamic amenorrhoea and polycystic ovarian morphology: a narrative review about an intriguing association.
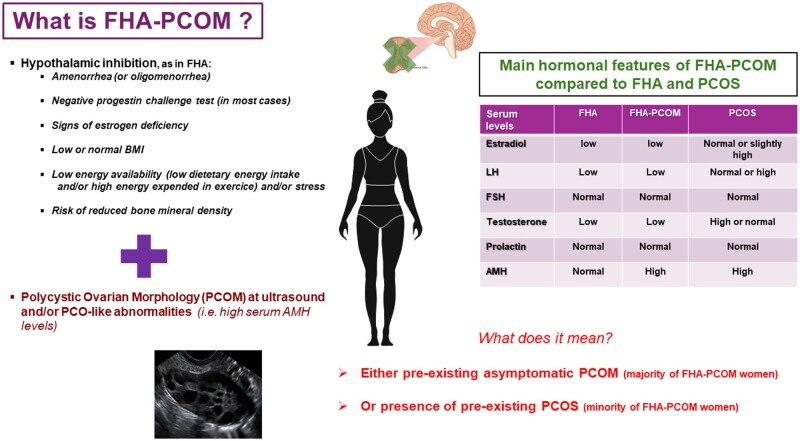
Background: Functional hypothalamic amenorrhoea (FHA) is responsible for 20-35% of all cases of secondary amenorrhoea and, thus, is the second most common cause of secondary amenorrhoea after polycystic ovary syndrome (PCOS). A high number of patients with FHA reveal polycystic ovarian morphology (PCOM) on ultrasound. The combination of amenorrhoea and PCOM can lead to confusion. First, amenorrhoeic women with PCOM fulfil the revised Rotterdam criteria and, thus, can easily be misdiagnosed with PCOS. Moreover, it has been claimed that some women with FHA and concomitant PCOM differ from those without PCOM in terms of endocrine regulation and metabolic traits.
Objective and rationale: The main focus of this article was on studies about FHA, which differentiated between patients with or without PCOM. The aim was to estimate the prevalence of PCOM and to look if it has an impact on pathophysiologic, diagnostic and therapeutic issues as well as on long-term consequences.
Search methods: Peer review original and review articles were selected from PubMed searches for this review. Searches were performed using the search terms 'polycystic AND functional hypothalamic amenorrhoea'. The reference lists of publications found were searched for relevant additional studies. The inclusion criteria for publications were: English language, patients' age ≥ 18 years, year of publication >1980, original studies, validated diagnosis of FHA, and validated diagnosis of PCOM using transvaginal ultrasound.
Outcomes: The prevalence of PCOM in women with FHA varied from 41.9% to 46.7%, which is higher than in healthy non-PCOS controls. Hypothetically, the high prevalence might be due to a mixture of silent PCOM, as in the general population, and pre-existing PCOS. Several differences in metabolic and hormonal parameters were found between FHA-PCOM and FHA-non-PCOM patients. While oestrogen deficiency is common to both groups of patients, FHA-PCOM patients have a higher BMI, higher levels of anti-Müllerian hormone (AMH) and testosterone, a higher increase in LH in the course of a GnRH test, and lower sex hormone binding globulin (SHBG) levels than FHA-non-PCOM patients. The differential diagnosis between FHA-PCOM and PCOS, especially PCOS phenotype D (PCOM and oligo-/anovulation without hyperandrogenism), can be challenging. Several parameters have been suggested, which are helpful though not absolutely reliable. They include the typical causes for FHA (excessive exercise, energy deficit, and/or psychological stress), the serum levels of LH, testosterone, and SHBG, as well as the progestin challenge test. Whether FHA-PCOM has a different risk profile for long-term consequences concerning patients' metabolic and cardiovascular situation as well as their bone mass, is unclear. Concerning therapeutic aspects, there are only few data about FHA-PCOM compared to FHA-non-PCOM. To treat anovulation, the use of pulsatile GnRH treatment seems to be equally effective in both groups. Similar to FHA-non-PCOM patients, pulsatile GnRH therapy would be more efficient than exogenous gonadotropins in FHA-PCOM patients.
Wider implications: Women with FHA-PCOM present a special sub-population of FHA patients. The diagnostic pitfall of FHA-PCOM should be emphasized in clinical guidelines about FHA and PCOS. The fact that almost half of the women with FHA have an ovarian follicle excess (i.e. PCOM) in face of low gonadotropin serum levels suggests that the intra-ovarian regulation of folliculogenesis is subject to individual variations, for unknown reasons, either genetic or epigenetic. Further studies are needed to investigate this hypothesis.
期刊介绍:
Human Reproduction Update is the leading journal in its field, boasting a Journal Impact FactorTM of 13.3 and ranked first in Obstetrics & Gynecology and Reproductive Biology (Source: Journal Citation ReportsTM from Clarivate, 2023). It specializes in publishing comprehensive and systematic review articles covering various aspects of human reproductive physiology and medicine.
The journal prioritizes basic, transitional, and clinical topics related to reproduction, encompassing areas such as andrology, embryology, infertility, gynaecology, pregnancy, reproductive endocrinology, reproductive epidemiology, reproductive genetics, reproductive immunology, and reproductive oncology. Human Reproduction Update is published on behalf of the European Society of Human Reproduction and Embryology (ESHRE), maintaining the highest scientific and editorial standards.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


