H Rhodes Hambrick, Nieko Punt, Kathryn Pavia, Tomoyuki Mizuno, Stuart L Goldstein, Sonya Tang Girdwood
{"title":"对接受持续肾脏替代疗法的儿童进行头孢吡肟的蒙特卡洛模拟,支持持续输注以达到目标。","authors":"H Rhodes Hambrick, Nieko Punt, Kathryn Pavia, Tomoyuki Mizuno, Stuart L Goldstein, Sonya Tang Girdwood","doi":"10.1186/s40560-024-00752-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sepsis is a leading cause of acute kidney injury requiring continuous kidney replacement therapy (CKRT) and CKRT can alter drug pharmacokinetics (PK). Cefepime is used commonly in critically ill children and is cleared by CKRT, yet data regarding cefepime PK and pharmacodynamic (PD) target attainment in children receiving CKRT are scarce, so we performed Monte Carlo simulations (MCS) of cefepime dosing strategies in children receiving CKRT.</p><p><strong>Methods: </strong>We developed a CKRT \"module\" in the precision dosing software Edsim++. The module was added into a pediatric cefepime PK model. 1000-fold MCS were performed using six dosing strategies in patients aged 2-25 years and ≥ 10 kg with differing residual kidney function (estimated glomerular filtration rate of 5 vs 30 mL/min/1.73 m<sup>2</sup>), CKRT prescriptions, (standard-dose total effluent flow of 2500 mL/h/1.73 m<sup>2</sup> vs high-dose of 8000 mL/h/1.73 m<sup>2</sup>), and fluid accumulation (0-30%). Probability of target attainment (PTA) was defined by percentage of patients with free concentrations exceeding bacterial minimum inhibitory concentration (MIC) for 100% of the dosing interval (100% fT > 1xMIC) and 4xMIC using an MIC of 8 mg/L for Pseudomonas aeruginosa.</p><p><strong>Results: </strong>Assuming standard-dose dialysis and minimal kidney function, > 90% PTA was achieved for 100% fT > 1x MIC with continuous infusions (CI) of 100-150 mg/kg/day (max 4/6 g) and 4-h infusions of 50 mg/kg (max 2 g), but > 90% PTA for 100% fT > 4x MIC was only achieved by 150 mg/kg CI. Decreased PTA was seen with less frequent dosing, shorter infusions, higher-dose CKRT, and higher residual kidney function.</p><p><strong>Conclusions: </strong>Our new CKRT-module was successfully added to an existing cefepime PK model for MCS in young patients on CKRT. When targeting 100% fT > 4xMIC or using higher-dose CKRT, CI would allow for higher PTA than intermittent dosing.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"12 1","pages":"38"},"PeriodicalIF":4.7000,"publicationDate":"2024-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11459894/pdf/","citationCount":"0","resultStr":"{\"title\":\"Monte Carlo simulations of cefepime in children receiving continuous kidney replacement therapy support continuous infusions for target attainment.\",\"authors\":\"H Rhodes Hambrick, Nieko Punt, Kathryn Pavia, Tomoyuki Mizuno, Stuart L Goldstein, Sonya Tang Girdwood\",\"doi\":\"10.1186/s40560-024-00752-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sepsis is a leading cause of acute kidney injury requiring continuous kidney replacement therapy (CKRT) and CKRT can alter drug pharmacokinetics (PK). Cefepime is used commonly in critically ill children and is cleared by CKRT, yet data regarding cefepime PK and pharmacodynamic (PD) target attainment in children receiving CKRT are scarce, so we performed Monte Carlo simulations (MCS) of cefepime dosing strategies in children receiving CKRT.</p><p><strong>Methods: </strong>We developed a CKRT \\\"module\\\" in the precision dosing software Edsim++. The module was added into a pediatric cefepime PK model. 1000-fold MCS were performed using six dosing strategies in patients aged 2-25 years and ≥ 10 kg with differing residual kidney function (estimated glomerular filtration rate of 5 vs 30 mL/min/1.73 m<sup>2</sup>), CKRT prescriptions, (standard-dose total effluent flow of 2500 mL/h/1.73 m<sup>2</sup> vs high-dose of 8000 mL/h/1.73 m<sup>2</sup>), and fluid accumulation (0-30%). Probability of target attainment (PTA) was defined by percentage of patients with free concentrations exceeding bacterial minimum inhibitory concentration (MIC) for 100% of the dosing interval (100% fT > 1xMIC) and 4xMIC using an MIC of 8 mg/L for Pseudomonas aeruginosa.</p><p><strong>Results: </strong>Assuming standard-dose dialysis and minimal kidney function, > 90% PTA was achieved for 100% fT > 1x MIC with continuous infusions (CI) of 100-150 mg/kg/day (max 4/6 g) and 4-h infusions of 50 mg/kg (max 2 g), but > 90% PTA for 100% fT > 4x MIC was only achieved by 150 mg/kg CI. Decreased PTA was seen with less frequent dosing, shorter infusions, higher-dose CKRT, and higher residual kidney function.</p><p><strong>Conclusions: </strong>Our new CKRT-module was successfully added to an existing cefepime PK model for MCS in young patients on CKRT. When targeting 100% fT > 4xMIC or using higher-dose CKRT, CI would allow for higher PTA than intermittent dosing.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"12 1\",\"pages\":\"38\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-10-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11459894/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-024-00752-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-024-00752-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:脓毒症是导致急性肾损伤的主要原因,需要进行持续肾脏替代治疗(CKRT),而CKRT会改变药物的药代动力学(PK)。头孢吡肟是重症儿童的常用药物,可通过 CKRT 清除,但有关接受 CKRT 儿童的头孢吡肟 PK 和药效学 (PD) 达标情况的数据却很少,因此我们对接受 CKRT 儿童的头孢吡肟给药策略进行了蒙特卡罗模拟 (MCS):方法:我们在精确给药软件 Edsim++ 中开发了一个 CKRT "模块"。方法:我们在精确给药软件 Edsim++ 中开发了 CKRT "模块",并将该模块添加到小儿头孢吡肟 PK 模型中。我们使用六种给药策略对 2-25 岁、体重≥ 10 kg 的患者进行了 1000 倍 MCS 分析,这些患者的残余肾功能(估计肾小球滤过率为 5 vs 30 mL/min/1.73 m2)、CKRT 处方(标准剂量总流出流量为 2500 mL/h/1.73 m2 vs 高剂量为 8000 mL/h/1.73 m2)和体液蓄积(0-30%)各不相同。达到目标的概率(PTA)是指在 100%的给药间隔内(100% fT > 1xMIC),游离浓度超过细菌最低抑菌浓度(MIC)的患者百分比,铜绿假单胞菌的 MIC 为 8 mg/L,则游离浓度为 4xMIC:假设采用标准剂量透析且肾功能极差,连续输注(CI)100-150 毫克/千克/天(最大 4/6 克)和 4 小时输注 50 毫克/千克(最大 2 克),100% fT > 1x MIC 的 PTA > 90%,但 100% fT > 4x MIC 的 PTA > 90%,只有 150 毫克/千克 CI 才能达到。用药次数少、输液时间短、CKRT 剂量大、残余肾功能高时,PTA 会降低:我们的新 CKRT 模块成功地添加到了现有的头孢吡肟 PK 模型中,用于治疗接受 CKRT 的年轻患者的 MCS。当目标值为 100% fT > 4xMIC 或使用较高剂量的 CKRT 时,CI 可使 PTA 高于间歇给药。
Monte Carlo simulations of cefepime in children receiving continuous kidney replacement therapy support continuous infusions for target attainment.
Background: Sepsis is a leading cause of acute kidney injury requiring continuous kidney replacement therapy (CKRT) and CKRT can alter drug pharmacokinetics (PK). Cefepime is used commonly in critically ill children and is cleared by CKRT, yet data regarding cefepime PK and pharmacodynamic (PD) target attainment in children receiving CKRT are scarce, so we performed Monte Carlo simulations (MCS) of cefepime dosing strategies in children receiving CKRT.
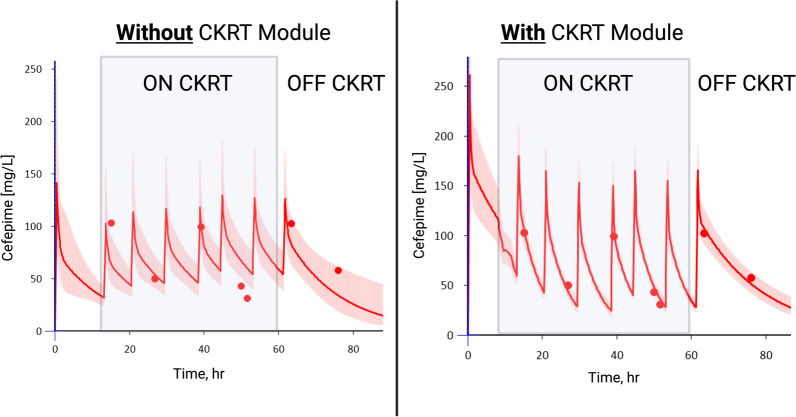
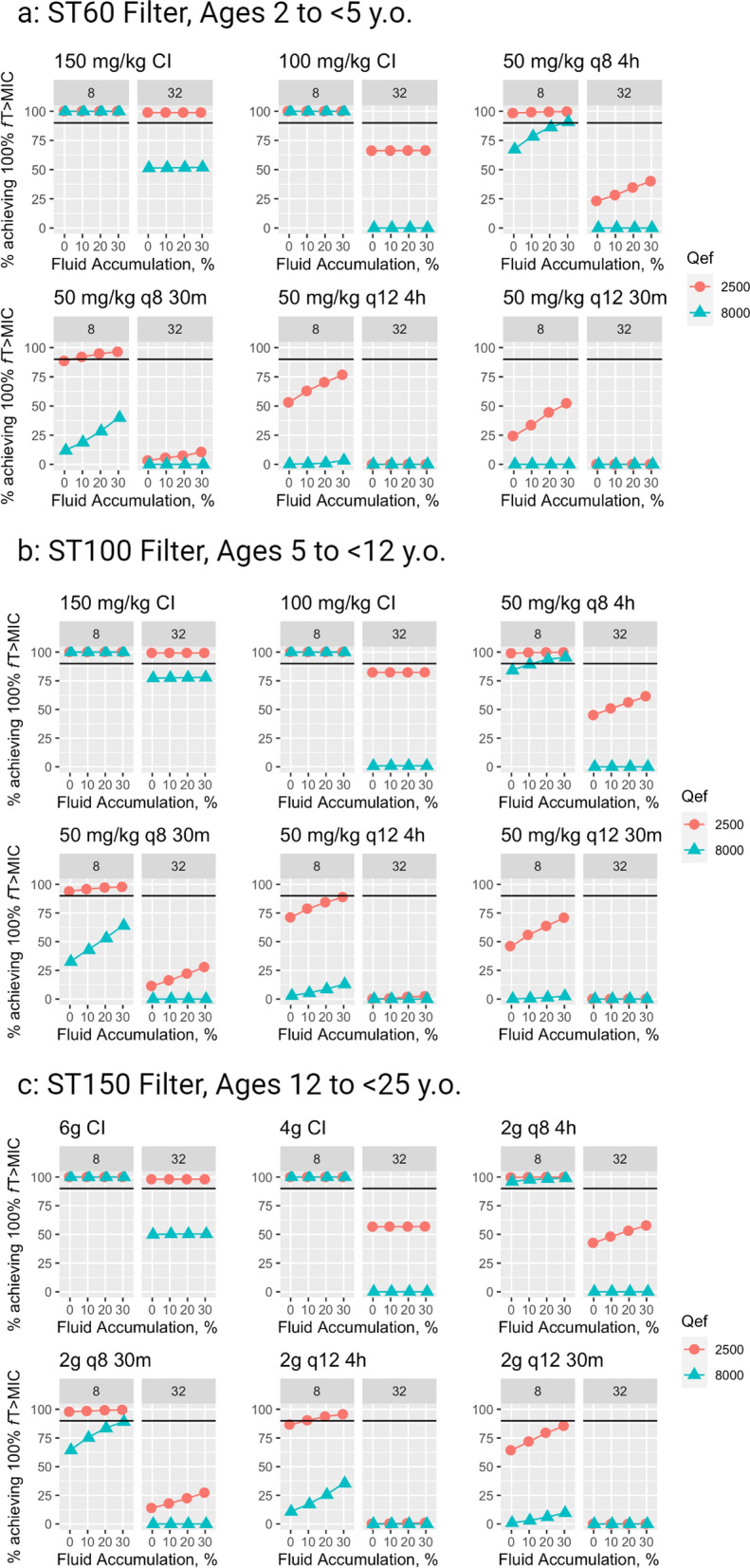
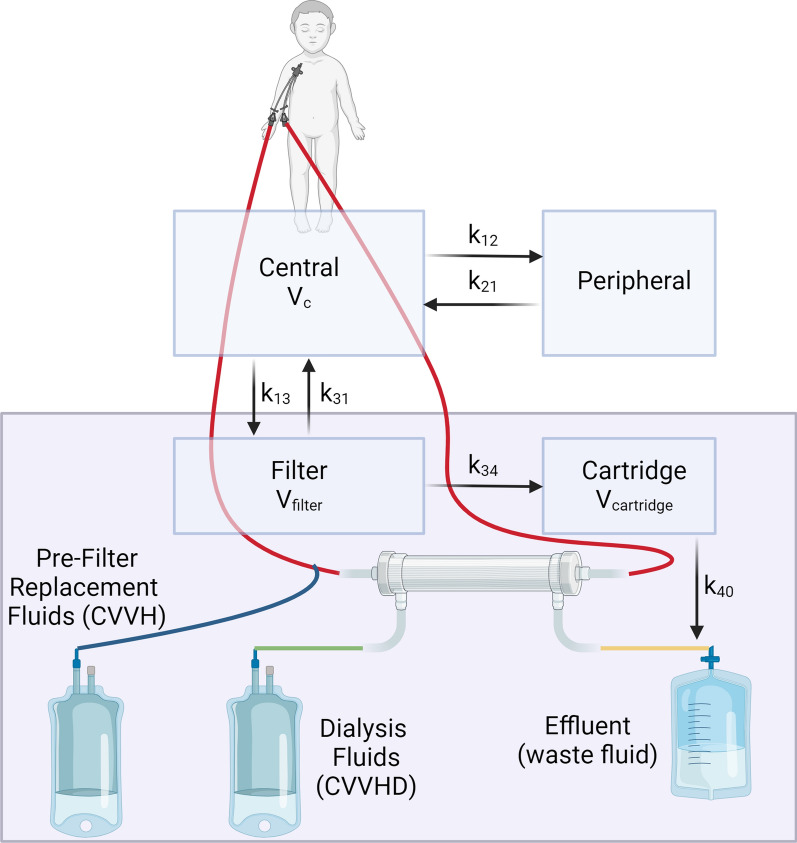
Methods: We developed a CKRT "module" in the precision dosing software Edsim++. The module was added into a pediatric cefepime PK model. 1000-fold MCS were performed using six dosing strategies in patients aged 2-25 years and ≥ 10 kg with differing residual kidney function (estimated glomerular filtration rate of 5 vs 30 mL/min/1.73 m2), CKRT prescriptions, (standard-dose total effluent flow of 2500 mL/h/1.73 m2 vs high-dose of 8000 mL/h/1.73 m2), and fluid accumulation (0-30%). Probability of target attainment (PTA) was defined by percentage of patients with free concentrations exceeding bacterial minimum inhibitory concentration (MIC) for 100% of the dosing interval (100% fT > 1xMIC) and 4xMIC using an MIC of 8 mg/L for Pseudomonas aeruginosa.
Results: Assuming standard-dose dialysis and minimal kidney function, > 90% PTA was achieved for 100% fT > 1x MIC with continuous infusions (CI) of 100-150 mg/kg/day (max 4/6 g) and 4-h infusions of 50 mg/kg (max 2 g), but > 90% PTA for 100% fT > 4x MIC was only achieved by 150 mg/kg CI. Decreased PTA was seen with less frequent dosing, shorter infusions, higher-dose CKRT, and higher residual kidney function.
Conclusions: Our new CKRT-module was successfully added to an existing cefepime PK model for MCS in young patients on CKRT. When targeting 100% fT > 4xMIC or using higher-dose CKRT, CI would allow for higher PTA than intermittent dosing.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


