Karoline Kallis, Christopher C. Conlin, Courtney Ollison, Michael E. Hahn, Rebecca Rakow-Penner, Anders M. Dale, Tyler M. Seibert
{"title":"用于对有临床意义的前列腺癌进行分类的定量 MRI 生物标记物:校准不同回波时间的可重复性。","authors":"Karoline Kallis, Christopher C. Conlin, Courtney Ollison, Michael E. Hahn, Rebecca Rakow-Penner, Anders M. Dale, Tyler M. Seibert","doi":"10.1002/acm2.14514","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Purpose</h3>\n \n <p>The purpose of the present study is to develop a calibration method to account for differences in echo times (TE) and facilitate the use of restriction spectrum imaging restriction score (RSIrs) as a quantitative biomarker for the detection of clinically significant prostate cancer (csPCa).</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study included 197 consecutive patients who underwent MRI and biopsy examination; 97 were diagnosed with csPCa (grade group ≥ 2). RSI data were acquired three times during the same session: twice at minimum TE ~75 ms and once at TE = 90 ms (TEmin<sub>1</sub>, TEmin<sub>2</sub>, and TE90, respectively). A linear regression model was determined to match the C-maps of TE90 to the reference C-maps of TEmin<sub>1</sub> within the interval ranging from 95th to 99th percentile of signal intensity within the prostate. RSIrs comparisons were made at the 98th percentile within each patient's prostate.</p>\n \n <p>We compared RSIrs from calibrated TE90 (RSIrs<sub>TE90corr</sub>) and uncorrected TE90 (RSIrs<sub>TE90</sub>) to RSIrs from reference TEmin<sub>1</sub> (RSIrs<sub>TEmin1</sub>) and repeated TEmin<sub>2</sub> (RSIrs<sub>TEmin2</sub>). Calibration performance was evaluated with sensitivity, specificity and area under the ROC curve (AUC).</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Scaling factors for C<sub>1</sub>, C<sub>2</sub>, C<sub>3</sub>, and C<sub>4</sub> were estimated as 1.68, 1.33, 1.02, and 1.13, respectively. In non-csPCa cases, the 98th percentile of RSIrs<sub>TEmin2</sub> and RSIrs<sub>TEmin1</sub> differed by 0.27 ± 0.86SI (mean ± standard deviation), whereas RSIrs<sub>TE90</sub> differed from RSIrs<sub>TEmin1</sub> by 1.82 ± 1.20SI. After calibration, this bias was reduced to -0.51 ± 1.21SI, representing a 72% reduction in absolute error. For patients with csPCa, the difference was 0.54 ± 1.98SI between RSIrs<sub>TEmin2</sub> and RSIrs<sub>TEmin1</sub> and 2.28 ± 2.06SI between RSIrs<sub>TE90</sub> and RSIrs<sub>TEmin1</sub>. After calibration, the mean difference decreased to -1.03SI, a 55% reduction in absolute error. At the Youden index for patient-level classification of csPCa (8.94SI), RSIrs<sub>TEmin1</sub> has a sensitivity of 66% and a specificity of 72%.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The proposed linear calibration method produces similar quantitative biomarker values for acquisitions with different TE, reducing TE-induced error by 72% and 55% for non-csPCa and csPCa, respectively.</p>\n </section>\n </div>","PeriodicalId":14989,"journal":{"name":"Journal of Applied Clinical Medical Physics","volume":"25 11","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2024-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11539966/pdf/","citationCount":"0","resultStr":"{\"title\":\"Quantitative MRI biomarker for classification of clinically significant prostate cancer: Calibration for reproducibility across echo times\",\"authors\":\"Karoline Kallis, Christopher C. Conlin, Courtney Ollison, Michael E. Hahn, Rebecca Rakow-Penner, Anders M. Dale, Tyler M. Seibert\",\"doi\":\"10.1002/acm2.14514\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Purpose</h3>\\n \\n <p>The purpose of the present study is to develop a calibration method to account for differences in echo times (TE) and facilitate the use of restriction spectrum imaging restriction score (RSIrs) as a quantitative biomarker for the detection of clinically significant prostate cancer (csPCa).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This study included 197 consecutive patients who underwent MRI and biopsy examination; 97 were diagnosed with csPCa (grade group ≥ 2). RSI data were acquired three times during the same session: twice at minimum TE ~75 ms and once at TE = 90 ms (TEmin<sub>1</sub>, TEmin<sub>2</sub>, and TE90, respectively). A linear regression model was determined to match the C-maps of TE90 to the reference C-maps of TEmin<sub>1</sub> within the interval ranging from 95th to 99th percentile of signal intensity within the prostate. RSIrs comparisons were made at the 98th percentile within each patient's prostate.</p>\\n \\n <p>We compared RSIrs from calibrated TE90 (RSIrs<sub>TE90corr</sub>) and uncorrected TE90 (RSIrs<sub>TE90</sub>) to RSIrs from reference TEmin<sub>1</sub> (RSIrs<sub>TEmin1</sub>) and repeated TEmin<sub>2</sub> (RSIrs<sub>TEmin2</sub>). Calibration performance was evaluated with sensitivity, specificity and area under the ROC curve (AUC).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Scaling factors for C<sub>1</sub>, C<sub>2</sub>, C<sub>3</sub>, and C<sub>4</sub> were estimated as 1.68, 1.33, 1.02, and 1.13, respectively. In non-csPCa cases, the 98th percentile of RSIrs<sub>TEmin2</sub> and RSIrs<sub>TEmin1</sub> differed by 0.27 ± 0.86SI (mean ± standard deviation), whereas RSIrs<sub>TE90</sub> differed from RSIrs<sub>TEmin1</sub> by 1.82 ± 1.20SI. After calibration, this bias was reduced to -0.51 ± 1.21SI, representing a 72% reduction in absolute error. For patients with csPCa, the difference was 0.54 ± 1.98SI between RSIrs<sub>TEmin2</sub> and RSIrs<sub>TEmin1</sub> and 2.28 ± 2.06SI between RSIrs<sub>TE90</sub> and RSIrs<sub>TEmin1</sub>. After calibration, the mean difference decreased to -1.03SI, a 55% reduction in absolute error. At the Youden index for patient-level classification of csPCa (8.94SI), RSIrs<sub>TEmin1</sub> has a sensitivity of 66% and a specificity of 72%.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>The proposed linear calibration method produces similar quantitative biomarker values for acquisitions with different TE, reducing TE-induced error by 72% and 55% for non-csPCa and csPCa, respectively.</p>\\n </section>\\n </div>\",\"PeriodicalId\":14989,\"journal\":{\"name\":\"Journal of Applied Clinical Medical Physics\",\"volume\":\"25 11\",\"pages\":\"\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-10-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11539966/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Applied Clinical Medical Physics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/acm2.14514\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Applied Clinical Medical Physics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/acm2.14514","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Quantitative MRI biomarker for classification of clinically significant prostate cancer: Calibration for reproducibility across echo times
Purpose
The purpose of the present study is to develop a calibration method to account for differences in echo times (TE) and facilitate the use of restriction spectrum imaging restriction score (RSIrs) as a quantitative biomarker for the detection of clinically significant prostate cancer (csPCa).
Methods
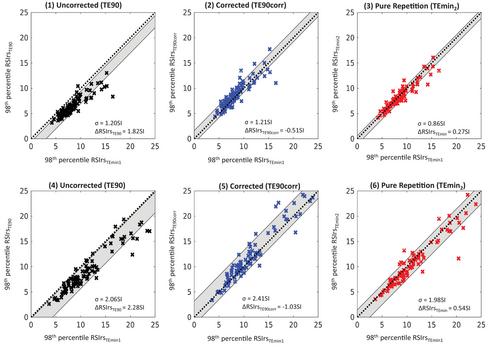
This study included 197 consecutive patients who underwent MRI and biopsy examination; 97 were diagnosed with csPCa (grade group ≥ 2). RSI data were acquired three times during the same session: twice at minimum TE ~75 ms and once at TE = 90 ms (TEmin1, TEmin2, and TE90, respectively). A linear regression model was determined to match the C-maps of TE90 to the reference C-maps of TEmin1 within the interval ranging from 95th to 99th percentile of signal intensity within the prostate. RSIrs comparisons were made at the 98th percentile within each patient's prostate.
We compared RSIrs from calibrated TE90 (RSIrsTE90corr) and uncorrected TE90 (RSIrsTE90) to RSIrs from reference TEmin1 (RSIrsTEmin1) and repeated TEmin2 (RSIrsTEmin2). Calibration performance was evaluated with sensitivity, specificity and area under the ROC curve (AUC).
Results
Scaling factors for C1, C2, C3, and C4 were estimated as 1.68, 1.33, 1.02, and 1.13, respectively. In non-csPCa cases, the 98th percentile of RSIrsTEmin2 and RSIrsTEmin1 differed by 0.27 ± 0.86SI (mean ± standard deviation), whereas RSIrsTE90 differed from RSIrsTEmin1 by 1.82 ± 1.20SI. After calibration, this bias was reduced to -0.51 ± 1.21SI, representing a 72% reduction in absolute error. For patients with csPCa, the difference was 0.54 ± 1.98SI between RSIrsTEmin2 and RSIrsTEmin1 and 2.28 ± 2.06SI between RSIrsTE90 and RSIrsTEmin1. After calibration, the mean difference decreased to -1.03SI, a 55% reduction in absolute error. At the Youden index for patient-level classification of csPCa (8.94SI), RSIrsTEmin1 has a sensitivity of 66% and a specificity of 72%.
Conclusions
The proposed linear calibration method produces similar quantitative biomarker values for acquisitions with different TE, reducing TE-induced error by 72% and 55% for non-csPCa and csPCa, respectively.
期刊介绍:
Journal of Applied Clinical Medical Physics is an international Open Access publication dedicated to clinical medical physics. JACMP welcomes original contributions dealing with all aspects of medical physics from scientists working in the clinical medical physics around the world. JACMP accepts only online submission.
JACMP will publish:
-Original Contributions: Peer-reviewed, investigations that represent new and significant contributions to the field. Recommended word count: up to 7500.
-Review Articles: Reviews of major areas or sub-areas in the field of clinical medical physics. These articles may be of any length and are peer reviewed.
-Technical Notes: These should be no longer than 3000 words, including key references.
-Letters to the Editor: Comments on papers published in JACMP or on any other matters of interest to clinical medical physics. These should not be more than 1250 (including the literature) and their publication is only based on the decision of the editor, who occasionally asks experts on the merit of the contents.
-Book Reviews: The editorial office solicits Book Reviews.
-Announcements of Forthcoming Meetings: The Editor may provide notice of forthcoming meetings, course offerings, and other events relevant to clinical medical physics.
-Parallel Opposed Editorial: We welcome topics relevant to clinical practice and medical physics profession. The contents can be controversial debate or opposed aspects of an issue. One author argues for the position and the other against. Each side of the debate contains an opening statement up to 800 words, followed by a rebuttal up to 500 words. Readers interested in participating in this series should contact the moderator with a proposed title and a short description of the topic

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


