{"title":"基于 CRISPR 的先天性免疫错误研究方法。","authors":"Joey H. Li","doi":"10.1002/ctm2.70021","DOIUrl":null,"url":null,"abstract":"<p>Inborn errors of immunity (IEI), formerly referred to as primary immunodeficiencies, affect millions of children worldwide.<span><sup>1</sup></span> Patients with IEI harbour germline mutations in genes responsible for immune system development or function, resulting in heightened susceptibility to infections as well as non-infectious sequelae such as increased incidence of malignancy or paradoxical autoimmunity.<span><sup>1</sup></span> While genetic testing is now a standard component of the workup for IEI, interpretation of results remains limited by our knowledge of causal pathogenic variants.<span><sup>2</sup></span> Currently, the primary method of identifying new variants associated with IEI depends on the clinical identification of a patient both bearing a novel mutation and presenting with severe or recurrent infections, pointing to a potential immune defect. While this approach has allowed us to greatly expand our identification of immunodeficient patients, the dependence on a chance encounter with a new patient represents a major barrier to identifying and providing prophylactic care for patients with unrecognized IEIs. Furthermore, this approach is limited to retrospectively identifying immunodeficient patients after they have already suffered from severe or recurrent infections. Therefore, a prospective laboratory-based screening method to identify putative IEI-associated genes followed by clinical validation of predicted pathogenic variants could improve our care for immunodeficient individuals.</p><p>To test a laboratory-based approach to prospectively identify and validate new IEI-associated gene variants, we focused on human natural killer (NK) cells and performed functional knockout screening of developmentally expressed transcription factors using CRISPR.<span><sup>3</sup></span> NK cells play a critical role during the early defense against viral infection via direct cytotoxicity against infected cells as well as the production of inflammatory mediators like interferon (IFN)-γ. This is highlighted by the increased and often fatal susceptibility to viral infection displayed by NK cell-deficient individuals.<span><sup>4</sup></span> However, the transcriptional regulators of human NK cell function that could lead to primary NK cell immunodeficiency when mutated remain poorly understood. We applied a CRISPR-Cas9 ribonucleoprotein (cRNP) electroporation protocol previously optimized by our group for primary immune cells to directly examine the role of 31 distinct transcription factors in mature primary human peripheral blood mononuclear cell (PBMC)-derived NK cells and identified a single gene, <i>MEF2C</i>, required for all tested effector functions.<span><sup>3, 5</sup></span> <i>MEF2C</i> knockout resulted in defective NK cell proliferation, cytotoxicity against tumor cells, degranulation, and production of inflammatory cytokines. We validated these findings by studying a small clinical cohort of two pediatric patients bearing pathogenic <i>MEF2C</i> point mutations resulting in MEF2C haploinsufficiency syndrome (MCHS), a recently characterized neurodevelopmental syndrome with no known associated immune defects.<span><sup>6</sup></span> Neither patient had known immune disorders but reported clinical histories of recurrent infections to varying degrees. Both patients displayed defective peripheral NK cell maturation with decreased mature cytotoxic cells identified as CD56<sup>dim</sup>CD16<sup>+</sup>, and we also observed deficient killing and production of the antiviral cytokine IFN-γ within the CD56<sup>dim</sup>CD16<sup>+</sup> subset. Due to the rarity of MCHS patients, we confirmed that <i>MEF2C</i> disruption is sufficient to induce NK cell-intrinsic functional defects by using Cas9 base editing to introduce a patient-like <i>MEF2C</i> point mutation in healthy donor NK cells. This approach phenocopied MCHS patient and <i>MEF2C</i> knockout NK cells, with base edited cells displaying defective proliferation and effector functions. Mechanistically, MEF2C was required to activate sterol regulatory element binding protein (SREBP)-dependent lipid metabolism in response to interleukin-15/mammalian target of rapamycin (mTOR) complex 1 signaling, and supplementation of CRISPR cRNP-edited or MCHS patient NK cells with the fatty acid oleate restored cytolytic activity <i>ex vivo</i>.</p><p>Our findings suggest that the neurodevelopmental disorder MCHS unexpectedly presents with NK cell defects. Case reports suggest MCHS patients may display increased susceptibility to infection, but the cause of these recurrent infections is unknown.<span><sup>7</sup></span> Other scenarios of combined neurodevelopmental and NK cell defects suggest that the central nervous system and immune compartment may share key developmental programs despite originating from distinct embryonic germ layers. For example, patients with heterozygous mutations in <i>BCL11B</i>, autism spectrum disorders, or MeCP2 duplication/triplication syndrome have all been reported to present with NK cell developmental arrest, functional impairment, and defects in other immune compartments.<span><sup>8-10</sup></span> Mutations in multiple positive regulators of NK cell function identified by our initial CRISPR screen (<i>KLF3</i>, <i>NR4A2</i>, <i>SETBP1</i>, <i>ZEB2</i> [Mowat-Wilson syndrome] and <i>RORA</i>) are also associated with reported intellectual disability or neurodevelopmental disorders yet lack formally reported immune defects, suggesting that these gene variants may also represent unrecognized combined neurological and immune deficiency.<span><sup>3</sup></span> Mechanistically, recent studies suggest that type 1 cytokines like IFN-γ produced by meningeal T and NK cells can modulate brain circuitry to affect behaviour and seizure susceptibility by modulating inhibitory neuronal circuit activity such as homeostatic inhibitory GABA-ergic signalling in the prefrontal cortex.<span><sup>11, 12</sup></span> Immune deficiencies associated with pediatric neurological disorders may be particularly undertreated, as frequent infections in these patients could be mistakenly attributed to increased oral and pharyngeal secretions and impaired clearance rather than innate immune defects.<span><sup>13</sup></span> Therefore, further study will be crucial to better identify and care for these potentially immunodeficient patients.</p><p>To our knowledge, non-viral CRISPR screening of transcription factors has not previously been performed in primary human NK cells prior to this study, though a similar cRNP-based approach has been applied to primary human T cells to identify new transcriptional drivers of regulatory T cell function.<span><sup>14</sup></span> Additionally, our approach provides a foundation for applying Cas9 base editing to understand cell-intrinsic roles of single gene defects when patient samples are limited. Identifying sufficient numbers of patients bearing a specific point mutation can be difficult, particularly with rare IEIs. To overcome these clinical limitations, Cas9 base editing can be applied to model the effects of rare patient point mutations at larger sample sizes by using healthy donor PBMCs. While studies using base-edited PBMCs are limited to examining gene function in mature peripheral immune cells, the effects of gene variants on immune cell development can instead be examined by base-editing CD34<sup>+</sup> hematopoietic stem cells. This approach has been previously performed to identify new gene variants that disrupt hematopoiesis as well as therapeutically to correct hematologic disorders like sickle cell anaemia or CD3δ severe combined immunodeficiency.<span><sup>15, 16</sup></span> New techniques to overexpress genes directly from the endogenous promoter using CRISPR activation (CRISPRa) offer another angle to interrogate gene function, either through direct overexpression of the affected gene or overexpression of downstream targets or enzymes to rescue the original defect. For example, while we show that oleate supplementation can restore MEF2C-deficient NK cell function, overexpression of the key oleate-producing enzyme stearoyl-CoA desaturase (SCD) could potentially also rescue MCHS-associated NK cell defects. While the lentiviral introduction of CRISPRa has been used to examine gene function in primary human T cells, non-viral CRISPRa expression offers an attractive alternative in immune cell types such as NK cells that are more resistant to viral transduction.<span><sup>17, 18</sup></span> Together, these CRISPR tools applied to primary human immune cells have high potential to reveal the pathogenicity of putative gene variants associated with inborn errors of immunity while overcoming the challenges of identifying and recruiting large numbers of rare patients (Figure 1).</p><p>As our clinical toolbox for treating immune disorders evolves, identifying more patients with IEI will become increasingly critical to effectively bring these therapies to bear. Our findings highlight the utility of targeted CRISPR cRNP screening and base editing in primary human immune cells to accurately predict and clinically validate a new NK cell immunodeficiency, an approach that can likely be leveraged in other primary human immune cells together with advanced CRISPR tools to identify new IEIs.</p><p>N/A</p><p>The author declares no conflict of interest.</p><p>N/A</p>","PeriodicalId":10189,"journal":{"name":"Clinical and Translational Medicine","volume":"14 10","pages":""},"PeriodicalIF":7.9000,"publicationDate":"2024-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11456690/pdf/","citationCount":"0","resultStr":"{\"title\":\"CRISPR-based approaches for studying inborn errors of immunity\",\"authors\":\"Joey H. Li\",\"doi\":\"10.1002/ctm2.70021\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Inborn errors of immunity (IEI), formerly referred to as primary immunodeficiencies, affect millions of children worldwide.<span><sup>1</sup></span> Patients with IEI harbour germline mutations in genes responsible for immune system development or function, resulting in heightened susceptibility to infections as well as non-infectious sequelae such as increased incidence of malignancy or paradoxical autoimmunity.<span><sup>1</sup></span> While genetic testing is now a standard component of the workup for IEI, interpretation of results remains limited by our knowledge of causal pathogenic variants.<span><sup>2</sup></span> Currently, the primary method of identifying new variants associated with IEI depends on the clinical identification of a patient both bearing a novel mutation and presenting with severe or recurrent infections, pointing to a potential immune defect. While this approach has allowed us to greatly expand our identification of immunodeficient patients, the dependence on a chance encounter with a new patient represents a major barrier to identifying and providing prophylactic care for patients with unrecognized IEIs. Furthermore, this approach is limited to retrospectively identifying immunodeficient patients after they have already suffered from severe or recurrent infections. Therefore, a prospective laboratory-based screening method to identify putative IEI-associated genes followed by clinical validation of predicted pathogenic variants could improve our care for immunodeficient individuals.</p><p>To test a laboratory-based approach to prospectively identify and validate new IEI-associated gene variants, we focused on human natural killer (NK) cells and performed functional knockout screening of developmentally expressed transcription factors using CRISPR.<span><sup>3</sup></span> NK cells play a critical role during the early defense against viral infection via direct cytotoxicity against infected cells as well as the production of inflammatory mediators like interferon (IFN)-γ. This is highlighted by the increased and often fatal susceptibility to viral infection displayed by NK cell-deficient individuals.<span><sup>4</sup></span> However, the transcriptional regulators of human NK cell function that could lead to primary NK cell immunodeficiency when mutated remain poorly understood. We applied a CRISPR-Cas9 ribonucleoprotein (cRNP) electroporation protocol previously optimized by our group for primary immune cells to directly examine the role of 31 distinct transcription factors in mature primary human peripheral blood mononuclear cell (PBMC)-derived NK cells and identified a single gene, <i>MEF2C</i>, required for all tested effector functions.<span><sup>3, 5</sup></span> <i>MEF2C</i> knockout resulted in defective NK cell proliferation, cytotoxicity against tumor cells, degranulation, and production of inflammatory cytokines. We validated these findings by studying a small clinical cohort of two pediatric patients bearing pathogenic <i>MEF2C</i> point mutations resulting in MEF2C haploinsufficiency syndrome (MCHS), a recently characterized neurodevelopmental syndrome with no known associated immune defects.<span><sup>6</sup></span> Neither patient had known immune disorders but reported clinical histories of recurrent infections to varying degrees. Both patients displayed defective peripheral NK cell maturation with decreased mature cytotoxic cells identified as CD56<sup>dim</sup>CD16<sup>+</sup>, and we also observed deficient killing and production of the antiviral cytokine IFN-γ within the CD56<sup>dim</sup>CD16<sup>+</sup> subset. Due to the rarity of MCHS patients, we confirmed that <i>MEF2C</i> disruption is sufficient to induce NK cell-intrinsic functional defects by using Cas9 base editing to introduce a patient-like <i>MEF2C</i> point mutation in healthy donor NK cells. This approach phenocopied MCHS patient and <i>MEF2C</i> knockout NK cells, with base edited cells displaying defective proliferation and effector functions. Mechanistically, MEF2C was required to activate sterol regulatory element binding protein (SREBP)-dependent lipid metabolism in response to interleukin-15/mammalian target of rapamycin (mTOR) complex 1 signaling, and supplementation of CRISPR cRNP-edited or MCHS patient NK cells with the fatty acid oleate restored cytolytic activity <i>ex vivo</i>.</p><p>Our findings suggest that the neurodevelopmental disorder MCHS unexpectedly presents with NK cell defects. Case reports suggest MCHS patients may display increased susceptibility to infection, but the cause of these recurrent infections is unknown.<span><sup>7</sup></span> Other scenarios of combined neurodevelopmental and NK cell defects suggest that the central nervous system and immune compartment may share key developmental programs despite originating from distinct embryonic germ layers. For example, patients with heterozygous mutations in <i>BCL11B</i>, autism spectrum disorders, or MeCP2 duplication/triplication syndrome have all been reported to present with NK cell developmental arrest, functional impairment, and defects in other immune compartments.<span><sup>8-10</sup></span> Mutations in multiple positive regulators of NK cell function identified by our initial CRISPR screen (<i>KLF3</i>, <i>NR4A2</i>, <i>SETBP1</i>, <i>ZEB2</i> [Mowat-Wilson syndrome] and <i>RORA</i>) are also associated with reported intellectual disability or neurodevelopmental disorders yet lack formally reported immune defects, suggesting that these gene variants may also represent unrecognized combined neurological and immune deficiency.<span><sup>3</sup></span> Mechanistically, recent studies suggest that type 1 cytokines like IFN-γ produced by meningeal T and NK cells can modulate brain circuitry to affect behaviour and seizure susceptibility by modulating inhibitory neuronal circuit activity such as homeostatic inhibitory GABA-ergic signalling in the prefrontal cortex.<span><sup>11, 12</sup></span> Immune deficiencies associated with pediatric neurological disorders may be particularly undertreated, as frequent infections in these patients could be mistakenly attributed to increased oral and pharyngeal secretions and impaired clearance rather than innate immune defects.<span><sup>13</sup></span> Therefore, further study will be crucial to better identify and care for these potentially immunodeficient patients.</p><p>To our knowledge, non-viral CRISPR screening of transcription factors has not previously been performed in primary human NK cells prior to this study, though a similar cRNP-based approach has been applied to primary human T cells to identify new transcriptional drivers of regulatory T cell function.<span><sup>14</sup></span> Additionally, our approach provides a foundation for applying Cas9 base editing to understand cell-intrinsic roles of single gene defects when patient samples are limited. Identifying sufficient numbers of patients bearing a specific point mutation can be difficult, particularly with rare IEIs. To overcome these clinical limitations, Cas9 base editing can be applied to model the effects of rare patient point mutations at larger sample sizes by using healthy donor PBMCs. While studies using base-edited PBMCs are limited to examining gene function in mature peripheral immune cells, the effects of gene variants on immune cell development can instead be examined by base-editing CD34<sup>+</sup> hematopoietic stem cells. This approach has been previously performed to identify new gene variants that disrupt hematopoiesis as well as therapeutically to correct hematologic disorders like sickle cell anaemia or CD3δ severe combined immunodeficiency.<span><sup>15, 16</sup></span> New techniques to overexpress genes directly from the endogenous promoter using CRISPR activation (CRISPRa) offer another angle to interrogate gene function, either through direct overexpression of the affected gene or overexpression of downstream targets or enzymes to rescue the original defect. For example, while we show that oleate supplementation can restore MEF2C-deficient NK cell function, overexpression of the key oleate-producing enzyme stearoyl-CoA desaturase (SCD) could potentially also rescue MCHS-associated NK cell defects. While the lentiviral introduction of CRISPRa has been used to examine gene function in primary human T cells, non-viral CRISPRa expression offers an attractive alternative in immune cell types such as NK cells that are more resistant to viral transduction.<span><sup>17, 18</sup></span> Together, these CRISPR tools applied to primary human immune cells have high potential to reveal the pathogenicity of putative gene variants associated with inborn errors of immunity while overcoming the challenges of identifying and recruiting large numbers of rare patients (Figure 1).</p><p>As our clinical toolbox for treating immune disorders evolves, identifying more patients with IEI will become increasingly critical to effectively bring these therapies to bear. Our findings highlight the utility of targeted CRISPR cRNP screening and base editing in primary human immune cells to accurately predict and clinically validate a new NK cell immunodeficiency, an approach that can likely be leveraged in other primary human immune cells together with advanced CRISPR tools to identify new IEIs.</p><p>N/A</p><p>The author declares no conflict of interest.</p><p>N/A</p>\",\"PeriodicalId\":10189,\"journal\":{\"name\":\"Clinical and Translational Medicine\",\"volume\":\"14 10\",\"pages\":\"\"},\"PeriodicalIF\":7.9000,\"publicationDate\":\"2024-10-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11456690/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70021\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70021","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
摘要
先天性免疫错误(IEI),以前被称为原发性免疫缺陷,影响着全球数百万儿童。1 IEI 患者体内负责免疫系统发育或功能的基因存在种系突变,导致对感染以及非感染性后遗症(如恶性肿瘤发病率增加或自相矛盾的自身免疫)的易感性增加。2 目前,鉴定与 IEI 相关的新变异的主要方法取决于临床鉴定,即患者既携带新变异,又出现严重或复发性感染,表明存在潜在的免疫缺陷。虽然这种方法使我们能够大大扩展对免疫缺陷患者的识别范围,但对新患者偶遇的依赖是识别未识别 IEI 患者并为其提供预防性治疗的主要障碍。此外,这种方法仅限于在免疫缺陷患者已经遭受严重或复发性感染后再对其进行回顾性识别。因此,采用一种前瞻性的实验室筛查方法来识别假定的 IEI 相关基因,然后对预测的致病变体进行临床验证,可以改善我们对免疫缺陷患者的治疗。为了测试一种前瞻性地识别和验证新的 IEI 相关基因变体的实验室方法,我们重点研究了人类自然杀伤(NK)细胞,并利用 CRISPR 对发育表达的转录因子进行了功能性基因敲除筛查。NK 细胞通过对感染细胞的直接细胞毒作用以及产生干扰素 (IFN)-γ 等炎症介质,在病毒感染的早期防御中发挥着关键作用。NK 细胞缺陷的个体对病毒感染的易感性增加,而且往往是致命的,这就凸显了这一点。4 然而,人类 NK 细胞功能的转录调节因子发生突变时可能导致原发性 NK 细胞免疫缺陷,但人们对这些调节因子的了解仍然很少。我们应用我们研究小组先前针对原代免疫细胞优化的 CRISPR-Cas9 核糖核蛋白(cRNP)电穿孔方案,直接检测了 31 个不同转录因子在成熟的原代人类外周血单核细胞(PBMC)衍生 NK 细胞中的作用,并确定了所有测试的效应功能都需要的单一基因 MEF2C。我们通过研究由两名携带致病性 MEF2C 点突变、导致 MEF2C 单倍体缺乏综合征(MCHS)的儿童患者组成的小型临床队列,验证了这些发现。这两名患者的外周 NK 细胞成熟度均有缺陷,CD56dimCD16+ 的成熟细胞毒性细胞减少,我们还观察到 CD56dimCD16+ 亚群的杀伤力和抗病毒细胞因子 IFN-γ 的产生不足。由于MCHS患者的罕见性,我们通过使用Cas9碱基编辑技术在健康供体NK细胞中引入类似患者的MEF2C点突变,证实MEF2C干扰足以诱导NK细胞内在功能缺陷。这种方法表征了MCHS患者和MEF2C基因敲除的NK细胞,碱基编辑的细胞显示出增殖和效应功能缺陷。从机理上讲,MEF2C需要激活固醇调节元件结合蛋白(SREBP)依赖的脂质代谢,以响应白细胞介素-15/哺乳动物雷帕霉素靶标(mTOR)复合物1的信号传导,用脂肪酸油酸补充CRISPR cRNP编辑的或MCHS患者的NK细胞可恢复体内外的细胞溶解活性。病例报告表明,MCHS 患者对感染的易感性可能会增加,但这些反复感染的原因尚不清楚。7 神经发育和 NK 细胞缺陷的其他合并情况表明,尽管中枢神经系统和免疫系统起源于不同的胚胎胚层,但它们可能共享关键的发育程序。例如,有报道称 BCL11B 杂合突变、自闭症谱系障碍或 MeCP2 复制/三复制综合征患者均表现为 NK 细胞发育停滞、功能障碍和其他免疫分区缺陷。
CRISPR-based approaches for studying inborn errors of immunity
Inborn errors of immunity (IEI), formerly referred to as primary immunodeficiencies, affect millions of children worldwide.1 Patients with IEI harbour germline mutations in genes responsible for immune system development or function, resulting in heightened susceptibility to infections as well as non-infectious sequelae such as increased incidence of malignancy or paradoxical autoimmunity.1 While genetic testing is now a standard component of the workup for IEI, interpretation of results remains limited by our knowledge of causal pathogenic variants.2 Currently, the primary method of identifying new variants associated with IEI depends on the clinical identification of a patient both bearing a novel mutation and presenting with severe or recurrent infections, pointing to a potential immune defect. While this approach has allowed us to greatly expand our identification of immunodeficient patients, the dependence on a chance encounter with a new patient represents a major barrier to identifying and providing prophylactic care for patients with unrecognized IEIs. Furthermore, this approach is limited to retrospectively identifying immunodeficient patients after they have already suffered from severe or recurrent infections. Therefore, a prospective laboratory-based screening method to identify putative IEI-associated genes followed by clinical validation of predicted pathogenic variants could improve our care for immunodeficient individuals.
To test a laboratory-based approach to prospectively identify and validate new IEI-associated gene variants, we focused on human natural killer (NK) cells and performed functional knockout screening of developmentally expressed transcription factors using CRISPR.3 NK cells play a critical role during the early defense against viral infection via direct cytotoxicity against infected cells as well as the production of inflammatory mediators like interferon (IFN)-γ. This is highlighted by the increased and often fatal susceptibility to viral infection displayed by NK cell-deficient individuals.4 However, the transcriptional regulators of human NK cell function that could lead to primary NK cell immunodeficiency when mutated remain poorly understood. We applied a CRISPR-Cas9 ribonucleoprotein (cRNP) electroporation protocol previously optimized by our group for primary immune cells to directly examine the role of 31 distinct transcription factors in mature primary human peripheral blood mononuclear cell (PBMC)-derived NK cells and identified a single gene, MEF2C, required for all tested effector functions.3, 5MEF2C knockout resulted in defective NK cell proliferation, cytotoxicity against tumor cells, degranulation, and production of inflammatory cytokines. We validated these findings by studying a small clinical cohort of two pediatric patients bearing pathogenic MEF2C point mutations resulting in MEF2C haploinsufficiency syndrome (MCHS), a recently characterized neurodevelopmental syndrome with no known associated immune defects.6 Neither patient had known immune disorders but reported clinical histories of recurrent infections to varying degrees. Both patients displayed defective peripheral NK cell maturation with decreased mature cytotoxic cells identified as CD56dimCD16+, and we also observed deficient killing and production of the antiviral cytokine IFN-γ within the CD56dimCD16+ subset. Due to the rarity of MCHS patients, we confirmed that MEF2C disruption is sufficient to induce NK cell-intrinsic functional defects by using Cas9 base editing to introduce a patient-like MEF2C point mutation in healthy donor NK cells. This approach phenocopied MCHS patient and MEF2C knockout NK cells, with base edited cells displaying defective proliferation and effector functions. Mechanistically, MEF2C was required to activate sterol regulatory element binding protein (SREBP)-dependent lipid metabolism in response to interleukin-15/mammalian target of rapamycin (mTOR) complex 1 signaling, and supplementation of CRISPR cRNP-edited or MCHS patient NK cells with the fatty acid oleate restored cytolytic activity ex vivo.
Our findings suggest that the neurodevelopmental disorder MCHS unexpectedly presents with NK cell defects. Case reports suggest MCHS patients may display increased susceptibility to infection, but the cause of these recurrent infections is unknown.7 Other scenarios of combined neurodevelopmental and NK cell defects suggest that the central nervous system and immune compartment may share key developmental programs despite originating from distinct embryonic germ layers. For example, patients with heterozygous mutations in BCL11B, autism spectrum disorders, or MeCP2 duplication/triplication syndrome have all been reported to present with NK cell developmental arrest, functional impairment, and defects in other immune compartments.8-10 Mutations in multiple positive regulators of NK cell function identified by our initial CRISPR screen (KLF3, NR4A2, SETBP1, ZEB2 [Mowat-Wilson syndrome] and RORA) are also associated with reported intellectual disability or neurodevelopmental disorders yet lack formally reported immune defects, suggesting that these gene variants may also represent unrecognized combined neurological and immune deficiency.3 Mechanistically, recent studies suggest that type 1 cytokines like IFN-γ produced by meningeal T and NK cells can modulate brain circuitry to affect behaviour and seizure susceptibility by modulating inhibitory neuronal circuit activity such as homeostatic inhibitory GABA-ergic signalling in the prefrontal cortex.11, 12 Immune deficiencies associated with pediatric neurological disorders may be particularly undertreated, as frequent infections in these patients could be mistakenly attributed to increased oral and pharyngeal secretions and impaired clearance rather than innate immune defects.13 Therefore, further study will be crucial to better identify and care for these potentially immunodeficient patients.
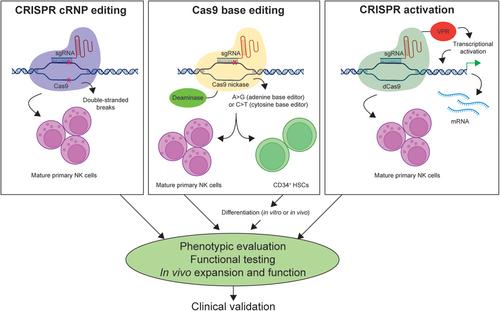
To our knowledge, non-viral CRISPR screening of transcription factors has not previously been performed in primary human NK cells prior to this study, though a similar cRNP-based approach has been applied to primary human T cells to identify new transcriptional drivers of regulatory T cell function.14 Additionally, our approach provides a foundation for applying Cas9 base editing to understand cell-intrinsic roles of single gene defects when patient samples are limited. Identifying sufficient numbers of patients bearing a specific point mutation can be difficult, particularly with rare IEIs. To overcome these clinical limitations, Cas9 base editing can be applied to model the effects of rare patient point mutations at larger sample sizes by using healthy donor PBMCs. While studies using base-edited PBMCs are limited to examining gene function in mature peripheral immune cells, the effects of gene variants on immune cell development can instead be examined by base-editing CD34+ hematopoietic stem cells. This approach has been previously performed to identify new gene variants that disrupt hematopoiesis as well as therapeutically to correct hematologic disorders like sickle cell anaemia or CD3δ severe combined immunodeficiency.15, 16 New techniques to overexpress genes directly from the endogenous promoter using CRISPR activation (CRISPRa) offer another angle to interrogate gene function, either through direct overexpression of the affected gene or overexpression of downstream targets or enzymes to rescue the original defect. For example, while we show that oleate supplementation can restore MEF2C-deficient NK cell function, overexpression of the key oleate-producing enzyme stearoyl-CoA desaturase (SCD) could potentially also rescue MCHS-associated NK cell defects. While the lentiviral introduction of CRISPRa has been used to examine gene function in primary human T cells, non-viral CRISPRa expression offers an attractive alternative in immune cell types such as NK cells that are more resistant to viral transduction.17, 18 Together, these CRISPR tools applied to primary human immune cells have high potential to reveal the pathogenicity of putative gene variants associated with inborn errors of immunity while overcoming the challenges of identifying and recruiting large numbers of rare patients (Figure 1).
As our clinical toolbox for treating immune disorders evolves, identifying more patients with IEI will become increasingly critical to effectively bring these therapies to bear. Our findings highlight the utility of targeted CRISPR cRNP screening and base editing in primary human immune cells to accurately predict and clinically validate a new NK cell immunodeficiency, an approach that can likely be leveraged in other primary human immune cells together with advanced CRISPR tools to identify new IEIs.
期刊介绍:
Clinical and Translational Medicine (CTM) is an international, peer-reviewed, open-access journal dedicated to accelerating the translation of preclinical research into clinical applications and fostering communication between basic and clinical scientists. It highlights the clinical potential and application of various fields including biotechnologies, biomaterials, bioengineering, biomarkers, molecular medicine, omics science, bioinformatics, immunology, molecular imaging, drug discovery, regulation, and health policy. With a focus on the bench-to-bedside approach, CTM prioritizes studies and clinical observations that generate hypotheses relevant to patients and diseases, guiding investigations in cellular and molecular medicine. The journal encourages submissions from clinicians, researchers, policymakers, and industry professionals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


