Thomas McDonnell, Philip A Kalra, Nicolas Vuilleumier, Paul Cockwell, David C Wheeler, Simon D S Fraser, Rosamonde E Banks, Maarten W Taal
{"title":"NURTuRE-CKD研究中原发性肾病诊断对预后的影响以及白蛋白尿的不同预测能力。","authors":"Thomas McDonnell, Philip A Kalra, Nicolas Vuilleumier, Paul Cockwell, David C Wheeler, Simon D S Fraser, Rosamonde E Banks, Maarten W Taal","doi":"10.1159/000541770","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The definition of CKD is broad, which neglects the heterogeneity of risk across primary renal diseases.</p><p><strong>Methods: </strong>The National Unified Renal Translational Research Enterprise (NURTuRE)-CKD is an ongoing UK, prospective multicenter cohort study of 2,996 adults with an eGFR of 15-59 mL/min/1.73 m2 or eGFR ≥60 mL/min/1.73 m2 with a urine albumin-to-creatinine ratio (uACR) >30 mg/mmol. Outcomes and predictive performance of eGFR and uACR were subcategorized by ERA-EDTA primary renal diagnosis (PRD) codes.</p><p><strong>Results: </strong>2,638 participants were included, with baseline median eGFR of 33.5 mL/min/1.73 m2 and uACR 29.8 mg/mmol. Over a median 49.2 months follow-up, 630 (23.9%) experienced kidney failure (KF), and 352 (13.3%) died before KF, the median eGFR slope was -1.97 mL/min/1.73 m2/year. There were significant differences in risk across the PRD, persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors (blood pressure, HbA1c, and renin-angiotensin-aldosterone system inhibitors). Diabetic kidney disease (DKD), glomerulonephritis, and familial/hereditary nephropathy were associated with the greatest risk, while tubulointerstitial disease and vasculitis carried a low risk of KF. eGFR had good predictive accuracy across all PRD. However, the addition of uACR showed variable benefit, depending on the PRD. The largest benefit was seen in vasculitis, renal vascular, and DKD groups, but uACR added no predictive value to the familial/hereditary group.</p><p><strong>Conclusion: </strong>Significant differences in the risk of kidney-related outcomes occurred across the various primary renal diagnoses persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors. Albuminuria's discriminatory ability as a biomarker of progression varies by diagnosis. CKD care should, therefore, take a personalized approach that always considers the primary renal diagnosis.</p><p><strong>Introduction: </strong>The definition of CKD is broad, which neglects the heterogeneity of risk across primary renal diseases.</p><p><strong>Methods: </strong>The National Unified Renal Translational Research Enterprise (NURTuRE)-CKD is an ongoing UK, prospective multicenter cohort study of 2,996 adults with an eGFR of 15-59 mL/min/1.73 m2 or eGFR ≥60 mL/min/1.73 m2 with a urine albumin-to-creatinine ratio (uACR) >30 mg/mmol. Outcomes and predictive performance of eGFR and uACR were subcategorized by ERA-EDTA primary renal diagnosis (PRD) codes.</p><p><strong>Results: </strong>2,638 participants were included, with baseline median eGFR of 33.5 mL/min/1.73 m2 and uACR 29.8 mg/mmol. Over a median 49.2 months follow-up, 630 (23.9%) experienced kidney failure (KF), and 352 (13.3%) died before KF, the median eGFR slope was -1.97 mL/min/1.73 m2/year. There were significant differences in risk across the PRD, persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors (blood pressure, HbA1c, and renin-angiotensin-aldosterone system inhibitors). Diabetic kidney disease (DKD), glomerulonephritis, and familial/hereditary nephropathy were associated with the greatest risk, while tubulointerstitial disease and vasculitis carried a low risk of KF. eGFR had good predictive accuracy across all PRD. However, the addition of uACR showed variable benefit, depending on the PRD. The largest benefit was seen in vasculitis, renal vascular, and DKD groups, but uACR added no predictive value to the familial/hereditary group.</p><p><strong>Conclusion: </strong>Significant differences in the risk of kidney-related outcomes occurred across the various primary renal diagnoses persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors. Albuminuria's discriminatory ability as a biomarker of progression varies by diagnosis. CKD care should, therefore, take a personalized approach that always considers the primary renal diagnosis.</p>","PeriodicalId":7570,"journal":{"name":"American Journal of Nephrology","volume":" ","pages":"1-12"},"PeriodicalIF":3.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11812588/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Primary Renal Diagnosis on Prognosis and the Varying Predictive Power of Albuminuria in the NURTuRE-CKD Study.\",\"authors\":\"Thomas McDonnell, Philip A Kalra, Nicolas Vuilleumier, Paul Cockwell, David C Wheeler, Simon D S Fraser, Rosamonde E Banks, Maarten W Taal\",\"doi\":\"10.1159/000541770\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The definition of CKD is broad, which neglects the heterogeneity of risk across primary renal diseases.</p><p><strong>Methods: </strong>The National Unified Renal Translational Research Enterprise (NURTuRE)-CKD is an ongoing UK, prospective multicenter cohort study of 2,996 adults with an eGFR of 15-59 mL/min/1.73 m2 or eGFR ≥60 mL/min/1.73 m2 with a urine albumin-to-creatinine ratio (uACR) >30 mg/mmol. Outcomes and predictive performance of eGFR and uACR were subcategorized by ERA-EDTA primary renal diagnosis (PRD) codes.</p><p><strong>Results: </strong>2,638 participants were included, with baseline median eGFR of 33.5 mL/min/1.73 m2 and uACR 29.8 mg/mmol. Over a median 49.2 months follow-up, 630 (23.9%) experienced kidney failure (KF), and 352 (13.3%) died before KF, the median eGFR slope was -1.97 mL/min/1.73 m2/year. There were significant differences in risk across the PRD, persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors (blood pressure, HbA1c, and renin-angiotensin-aldosterone system inhibitors). Diabetic kidney disease (DKD), glomerulonephritis, and familial/hereditary nephropathy were associated with the greatest risk, while tubulointerstitial disease and vasculitis carried a low risk of KF. eGFR had good predictive accuracy across all PRD. However, the addition of uACR showed variable benefit, depending on the PRD. The largest benefit was seen in vasculitis, renal vascular, and DKD groups, but uACR added no predictive value to the familial/hereditary group.</p><p><strong>Conclusion: </strong>Significant differences in the risk of kidney-related outcomes occurred across the various primary renal diagnoses persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors. Albuminuria's discriminatory ability as a biomarker of progression varies by diagnosis. CKD care should, therefore, take a personalized approach that always considers the primary renal diagnosis.</p><p><strong>Introduction: </strong>The definition of CKD is broad, which neglects the heterogeneity of risk across primary renal diseases.</p><p><strong>Methods: </strong>The National Unified Renal Translational Research Enterprise (NURTuRE)-CKD is an ongoing UK, prospective multicenter cohort study of 2,996 adults with an eGFR of 15-59 mL/min/1.73 m2 or eGFR ≥60 mL/min/1.73 m2 with a urine albumin-to-creatinine ratio (uACR) >30 mg/mmol. Outcomes and predictive performance of eGFR and uACR were subcategorized by ERA-EDTA primary renal diagnosis (PRD) codes.</p><p><strong>Results: </strong>2,638 participants were included, with baseline median eGFR of 33.5 mL/min/1.73 m2 and uACR 29.8 mg/mmol. Over a median 49.2 months follow-up, 630 (23.9%) experienced kidney failure (KF), and 352 (13.3%) died before KF, the median eGFR slope was -1.97 mL/min/1.73 m2/year. There were significant differences in risk across the PRD, persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors (blood pressure, HbA1c, and renin-angiotensin-aldosterone system inhibitors). Diabetic kidney disease (DKD), glomerulonephritis, and familial/hereditary nephropathy were associated with the greatest risk, while tubulointerstitial disease and vasculitis carried a low risk of KF. eGFR had good predictive accuracy across all PRD. However, the addition of uACR showed variable benefit, depending on the PRD. The largest benefit was seen in vasculitis, renal vascular, and DKD groups, but uACR added no predictive value to the familial/hereditary group.</p><p><strong>Conclusion: </strong>Significant differences in the risk of kidney-related outcomes occurred across the various primary renal diagnoses persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors. Albuminuria's discriminatory ability as a biomarker of progression varies by diagnosis. CKD care should, therefore, take a personalized approach that always considers the primary renal diagnosis.</p>\",\"PeriodicalId\":7570,\"journal\":{\"name\":\"American Journal of Nephrology\",\"volume\":\" \",\"pages\":\"1-12\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11812588/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Nephrology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1159/000541770\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000541770","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
The Impact of Primary Renal Diagnosis on Prognosis and the Varying Predictive Power of Albuminuria in the NURTuRE-CKD Study.
Introduction: The definition of CKD is broad, which neglects the heterogeneity of risk across primary renal diseases.
Methods: The National Unified Renal Translational Research Enterprise (NURTuRE)-CKD is an ongoing UK, prospective multicenter cohort study of 2,996 adults with an eGFR of 15-59 mL/min/1.73 m2 or eGFR ≥60 mL/min/1.73 m2 with a urine albumin-to-creatinine ratio (uACR) >30 mg/mmol. Outcomes and predictive performance of eGFR and uACR were subcategorized by ERA-EDTA primary renal diagnosis (PRD) codes.
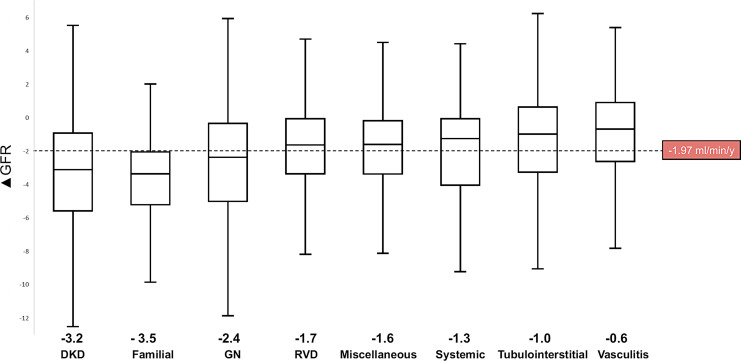
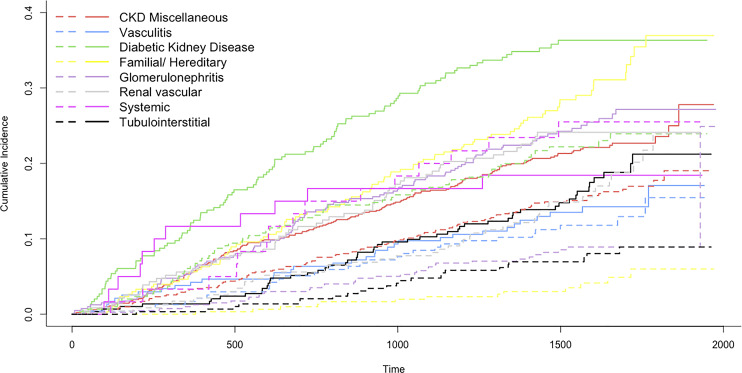
Results: 2,638 participants were included, with baseline median eGFR of 33.5 mL/min/1.73 m2 and uACR 29.8 mg/mmol. Over a median 49.2 months follow-up, 630 (23.9%) experienced kidney failure (KF), and 352 (13.3%) died before KF, the median eGFR slope was -1.97 mL/min/1.73 m2/year. There were significant differences in risk across the PRD, persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors (blood pressure, HbA1c, and renin-angiotensin-aldosterone system inhibitors). Diabetic kidney disease (DKD), glomerulonephritis, and familial/hereditary nephropathy were associated with the greatest risk, while tubulointerstitial disease and vasculitis carried a low risk of KF. eGFR had good predictive accuracy across all PRD. However, the addition of uACR showed variable benefit, depending on the PRD. The largest benefit was seen in vasculitis, renal vascular, and DKD groups, but uACR added no predictive value to the familial/hereditary group.
Conclusion: Significant differences in the risk of kidney-related outcomes occurred across the various primary renal diagnoses persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors. Albuminuria's discriminatory ability as a biomarker of progression varies by diagnosis. CKD care should, therefore, take a personalized approach that always considers the primary renal diagnosis.
Introduction: The definition of CKD is broad, which neglects the heterogeneity of risk across primary renal diseases.
Methods: The National Unified Renal Translational Research Enterprise (NURTuRE)-CKD is an ongoing UK, prospective multicenter cohort study of 2,996 adults with an eGFR of 15-59 mL/min/1.73 m2 or eGFR ≥60 mL/min/1.73 m2 with a urine albumin-to-creatinine ratio (uACR) >30 mg/mmol. Outcomes and predictive performance of eGFR and uACR were subcategorized by ERA-EDTA primary renal diagnosis (PRD) codes.
Results: 2,638 participants were included, with baseline median eGFR of 33.5 mL/min/1.73 m2 and uACR 29.8 mg/mmol. Over a median 49.2 months follow-up, 630 (23.9%) experienced kidney failure (KF), and 352 (13.3%) died before KF, the median eGFR slope was -1.97 mL/min/1.73 m2/year. There were significant differences in risk across the PRD, persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors (blood pressure, HbA1c, and renin-angiotensin-aldosterone system inhibitors). Diabetic kidney disease (DKD), glomerulonephritis, and familial/hereditary nephropathy were associated with the greatest risk, while tubulointerstitial disease and vasculitis carried a low risk of KF. eGFR had good predictive accuracy across all PRD. However, the addition of uACR showed variable benefit, depending on the PRD. The largest benefit was seen in vasculitis, renal vascular, and DKD groups, but uACR added no predictive value to the familial/hereditary group.
Conclusion: Significant differences in the risk of kidney-related outcomes occurred across the various primary renal diagnoses persisting after adjustment for age, sex, baseline eGFR, and modifiable risk factors. Albuminuria's discriminatory ability as a biomarker of progression varies by diagnosis. CKD care should, therefore, take a personalized approach that always considers the primary renal diagnosis.
期刊介绍:
The ''American Journal of Nephrology'' is a peer-reviewed journal that focuses on timely topics in both basic science and clinical research. Papers are divided into several sections, including:

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


