{"title":"评估在 Trendelenburg 体位下接受腹腔镜手术的患者的视神经鞘直径:一项前瞻性观察研究。","authors":"Burak Ömür, Bahadır Çiftçi, Pelin Karaaslan","doi":"10.5144/0256-4947.2024.319","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Trendelenburg position and pneumoperitoneum may cause cerebral edema and increased intracranial pressure. Non-invasive measurement of the diameter of the optic nerve sheath by ultrasonography can provide early recognition of intracranial pressure.</p><p><strong>Objective: </strong>Evaluate the optic nerve sheath diameter (ONSD) changes in patients who undergo laparoscopic surgery in the Trendelenburg position and make indirect conclusions about changes in intracranial pressure.</p><p><strong>Design: </strong>Prospective, observational.</p><p><strong>Setting: </strong>Laparoscopic surgeries.</p><p><strong>Patients and methods: </strong>Patients aged 18-75 years who underwent laparoscopic surgery in the Trendelenburg position under general anesthesia were included in our study. The ONSD was measured four times: Immediately after tracheal intubation, in the neutral position (baseline value) (T0), 10 minutes after pneumoperitoneum and Trendelenburg position (T1), 60 minutes after pneumoperitoneum and Trendelenburg position (T2), and 10 minutes after the pneumoperitoneum is terminated and placed in the neutral position (T3).</p><p><strong>Main outcome measures: </strong>Compare ONSD measured by ultrasonography at different times of surgery.</p><p><strong>Sample size: </strong>40.</p><p><strong>Results: </strong>Arterial carbon dioxide pressure increased with laparoscopy and Trendelenburg position in parallel with ONSD measurements and decreased again after returning to the neutral position. It was still higher than the baseline value at the T3. There was also a significant difference[a] between the measurement made at the T2 and the measurement made at T1. This difference showed that the prolongation of the Trendelenburg time was associated with an increase in ONSD. At the end of the operation it was observed that the decreased statistically significantly (T3) 10 minutes after the pneumoperitoneum was terminated and the position was corrected. However, the ONSD was still higher at the end of the operation (T3) compared to the baseline value measured at the beginning of the operation (T0).</p><p><strong>Conclusion: </strong>The ONSD increased in relation to Trendelenburg position and pneumoperitoneum. With these results, we think the ultrasonographic measurement of ONSD, a non-invasive method, can be used for clinical follow-up when performing laparoscopic surgery in the Trendelenburg position in cases requiring intracranial pressure monitoring.</p><p><strong>Limitations: </strong>There may be variations in the measurement of ONSD, even in the measurements of the same practitioner, as in all imaging with an ultrasonography device.</p>","PeriodicalId":93875,"journal":{"name":"Annals of Saudi medicine","volume":"44 5","pages":"319-328"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11454954/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of optic nerve sheath diameter in patients undergoing laparoscopic surgery in the Trendelenburg position: a prospective observational study.\",\"authors\":\"Burak Ömür, Bahadır Çiftçi, Pelin Karaaslan\",\"doi\":\"10.5144/0256-4947.2024.319\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Trendelenburg position and pneumoperitoneum may cause cerebral edema and increased intracranial pressure. Non-invasive measurement of the diameter of the optic nerve sheath by ultrasonography can provide early recognition of intracranial pressure.</p><p><strong>Objective: </strong>Evaluate the optic nerve sheath diameter (ONSD) changes in patients who undergo laparoscopic surgery in the Trendelenburg position and make indirect conclusions about changes in intracranial pressure.</p><p><strong>Design: </strong>Prospective, observational.</p><p><strong>Setting: </strong>Laparoscopic surgeries.</p><p><strong>Patients and methods: </strong>Patients aged 18-75 years who underwent laparoscopic surgery in the Trendelenburg position under general anesthesia were included in our study. The ONSD was measured four times: Immediately after tracheal intubation, in the neutral position (baseline value) (T0), 10 minutes after pneumoperitoneum and Trendelenburg position (T1), 60 minutes after pneumoperitoneum and Trendelenburg position (T2), and 10 minutes after the pneumoperitoneum is terminated and placed in the neutral position (T3).</p><p><strong>Main outcome measures: </strong>Compare ONSD measured by ultrasonography at different times of surgery.</p><p><strong>Sample size: </strong>40.</p><p><strong>Results: </strong>Arterial carbon dioxide pressure increased with laparoscopy and Trendelenburg position in parallel with ONSD measurements and decreased again after returning to the neutral position. It was still higher than the baseline value at the T3. There was also a significant difference[a] between the measurement made at the T2 and the measurement made at T1. This difference showed that the prolongation of the Trendelenburg time was associated with an increase in ONSD. At the end of the operation it was observed that the decreased statistically significantly (T3) 10 minutes after the pneumoperitoneum was terminated and the position was corrected. However, the ONSD was still higher at the end of the operation (T3) compared to the baseline value measured at the beginning of the operation (T0).</p><p><strong>Conclusion: </strong>The ONSD increased in relation to Trendelenburg position and pneumoperitoneum. With these results, we think the ultrasonographic measurement of ONSD, a non-invasive method, can be used for clinical follow-up when performing laparoscopic surgery in the Trendelenburg position in cases requiring intracranial pressure monitoring.</p><p><strong>Limitations: </strong>There may be variations in the measurement of ONSD, even in the measurements of the same practitioner, as in all imaging with an ultrasonography device.</p>\",\"PeriodicalId\":93875,\"journal\":{\"name\":\"Annals of Saudi medicine\",\"volume\":\"44 5\",\"pages\":\"319-328\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11454954/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Saudi medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5144/0256-4947.2024.319\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Saudi medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5144/0256-4947.2024.319","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/3 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Evaluation of optic nerve sheath diameter in patients undergoing laparoscopic surgery in the Trendelenburg position: a prospective observational study.
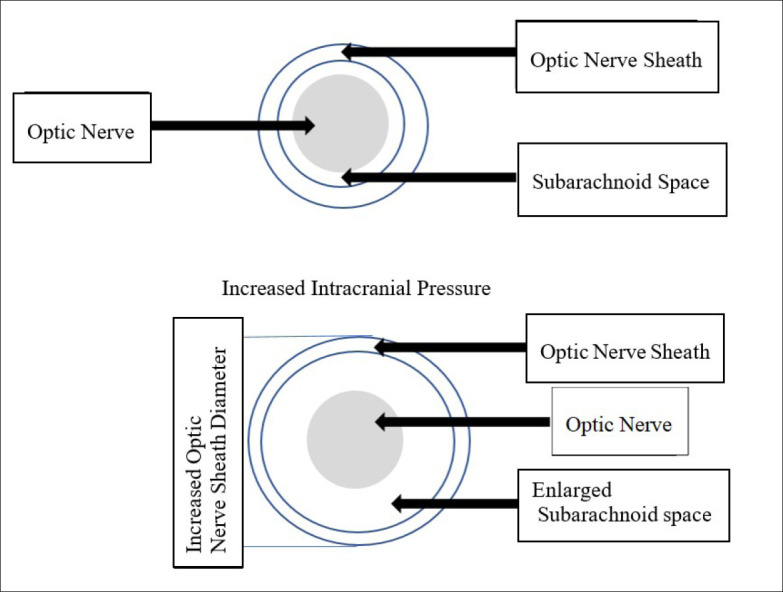
Background: The Trendelenburg position and pneumoperitoneum may cause cerebral edema and increased intracranial pressure. Non-invasive measurement of the diameter of the optic nerve sheath by ultrasonography can provide early recognition of intracranial pressure.
Objective: Evaluate the optic nerve sheath diameter (ONSD) changes in patients who undergo laparoscopic surgery in the Trendelenburg position and make indirect conclusions about changes in intracranial pressure.
Design: Prospective, observational.
Setting: Laparoscopic surgeries.
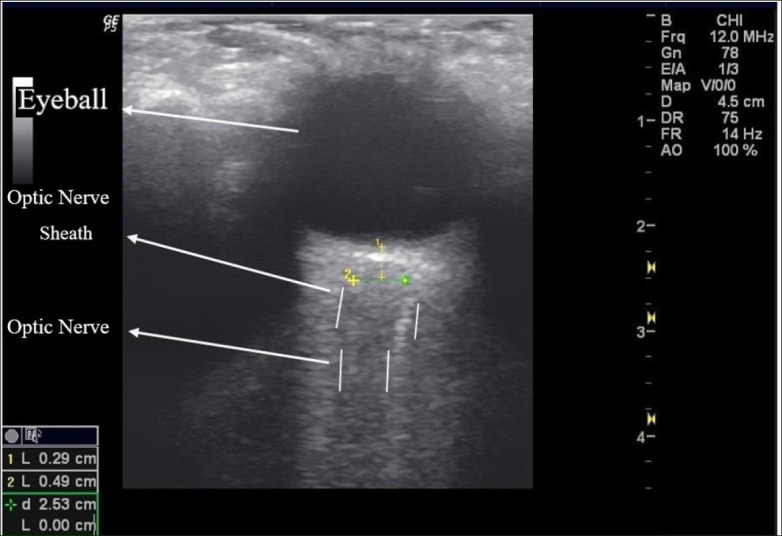
Patients and methods: Patients aged 18-75 years who underwent laparoscopic surgery in the Trendelenburg position under general anesthesia were included in our study. The ONSD was measured four times: Immediately after tracheal intubation, in the neutral position (baseline value) (T0), 10 minutes after pneumoperitoneum and Trendelenburg position (T1), 60 minutes after pneumoperitoneum and Trendelenburg position (T2), and 10 minutes after the pneumoperitoneum is terminated and placed in the neutral position (T3).
Main outcome measures: Compare ONSD measured by ultrasonography at different times of surgery.
Sample size: 40.
Results: Arterial carbon dioxide pressure increased with laparoscopy and Trendelenburg position in parallel with ONSD measurements and decreased again after returning to the neutral position. It was still higher than the baseline value at the T3. There was also a significant difference[a] between the measurement made at the T2 and the measurement made at T1. This difference showed that the prolongation of the Trendelenburg time was associated with an increase in ONSD. At the end of the operation it was observed that the decreased statistically significantly (T3) 10 minutes after the pneumoperitoneum was terminated and the position was corrected. However, the ONSD was still higher at the end of the operation (T3) compared to the baseline value measured at the beginning of the operation (T0).
Conclusion: The ONSD increased in relation to Trendelenburg position and pneumoperitoneum. With these results, we think the ultrasonographic measurement of ONSD, a non-invasive method, can be used for clinical follow-up when performing laparoscopic surgery in the Trendelenburg position in cases requiring intracranial pressure monitoring.
Limitations: There may be variations in the measurement of ONSD, even in the measurements of the same practitioner, as in all imaging with an ultrasonography device.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


