Anna Camporesi, Giulia Roveri, Luigi Vetrugno, Danilo Buonsenso, Valentina De Giorgis, Sara Costanzo, Ugo Maria Pierucci, Gloria Pelizzo
{"title":"对儿科患者采用不同麻醉诱导技术后发生肺不张的肺超声评估:一项倾向评分匹配的观察性研究。","authors":"Anna Camporesi, Giulia Roveri, Luigi Vetrugno, Danilo Buonsenso, Valentina De Giorgis, Sara Costanzo, Ugo Maria Pierucci, Gloria Pelizzo","doi":"10.1186/s44158-024-00206-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Atelectasis is a well-documented complication in pediatric patients undergoing general anesthesia. Its incidence varies significantly based on surgical procedures and anesthesia techniques. Inhalation induction, commonly used to avoid the discomfort of venipuncture, is suspected to cause higher rates of respiratory complications, including atelectasis, compared to intravenous induction. This study aimed to evaluate the impact of inhalation versus intravenous anesthesia induction on atelectasis formation in pediatric patients, as assessed by lung ultrasound (LUS).</p><p><strong>Methods: </strong>This propensity score-matched observational study was conducted at a tertiary pediatric hospital in Milan, Italy. Inclusion criteria were children ≤ 18 years undergoing elective surgery with general anesthesia. Patients were divided into inhalation and intravenous induction groups. LUS was performed before and after anesthesia induction to assess lung aeration. The primary endpoint was the global LUS score post-induction, with secondary endpoints including the incidence and distribution of atelectasis.</p><p><strong>Results: </strong>Of the 326 patients included, 65% underwent inhalation induction and 35% intravenous induction. The global LUS score was significantly higher in the inhalation group (12.0 vs. 4.0, p < 0.001). After propensity score matching (for age, presence of upper respiratory tract infection, duration of induction, and PEEP levels at induction), average treatment effect (ATE) of mask induction was 5.89 (95% CI, 3.21-8.58; p < 0.001) point on LUS global score and a coefficient of 0.35 (OR 1.41) for atelectasis.</p><p><strong>Discussion: </strong>Inhalation induction is associated with a higher incidence of atelectasis in pediatric patients also when we adjusted for clinically relevant covariates.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov identifier: NCT06069414.</p>","PeriodicalId":73597,"journal":{"name":"Journal of Anesthesia, Analgesia and Critical Care (Online)","volume":"4 1","pages":"69"},"PeriodicalIF":3.1000,"publicationDate":"2024-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11452973/pdf/","citationCount":"0","resultStr":"{\"title\":\"Lung ultrasound assessment of atelectasis following different anesthesia induction techniques in pediatric patients: a propensity score-matched, observational study.\",\"authors\":\"Anna Camporesi, Giulia Roveri, Luigi Vetrugno, Danilo Buonsenso, Valentina De Giorgis, Sara Costanzo, Ugo Maria Pierucci, Gloria Pelizzo\",\"doi\":\"10.1186/s44158-024-00206-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Atelectasis is a well-documented complication in pediatric patients undergoing general anesthesia. Its incidence varies significantly based on surgical procedures and anesthesia techniques. Inhalation induction, commonly used to avoid the discomfort of venipuncture, is suspected to cause higher rates of respiratory complications, including atelectasis, compared to intravenous induction. This study aimed to evaluate the impact of inhalation versus intravenous anesthesia induction on atelectasis formation in pediatric patients, as assessed by lung ultrasound (LUS).</p><p><strong>Methods: </strong>This propensity score-matched observational study was conducted at a tertiary pediatric hospital in Milan, Italy. Inclusion criteria were children ≤ 18 years undergoing elective surgery with general anesthesia. Patients were divided into inhalation and intravenous induction groups. LUS was performed before and after anesthesia induction to assess lung aeration. The primary endpoint was the global LUS score post-induction, with secondary endpoints including the incidence and distribution of atelectasis.</p><p><strong>Results: </strong>Of the 326 patients included, 65% underwent inhalation induction and 35% intravenous induction. The global LUS score was significantly higher in the inhalation group (12.0 vs. 4.0, p < 0.001). After propensity score matching (for age, presence of upper respiratory tract infection, duration of induction, and PEEP levels at induction), average treatment effect (ATE) of mask induction was 5.89 (95% CI, 3.21-8.58; p < 0.001) point on LUS global score and a coefficient of 0.35 (OR 1.41) for atelectasis.</p><p><strong>Discussion: </strong>Inhalation induction is associated with a higher incidence of atelectasis in pediatric patients also when we adjusted for clinically relevant covariates.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov identifier: NCT06069414.</p>\",\"PeriodicalId\":73597,\"journal\":{\"name\":\"Journal of Anesthesia, Analgesia and Critical Care (Online)\",\"volume\":\"4 1\",\"pages\":\"69\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-10-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11452973/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Anesthesia, Analgesia and Critical Care (Online)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44158-024-00206-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia, Analgesia and Critical Care (Online)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44158-024-00206-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Lung ultrasound assessment of atelectasis following different anesthesia induction techniques in pediatric patients: a propensity score-matched, observational study.
Introduction: Atelectasis is a well-documented complication in pediatric patients undergoing general anesthesia. Its incidence varies significantly based on surgical procedures and anesthesia techniques. Inhalation induction, commonly used to avoid the discomfort of venipuncture, is suspected to cause higher rates of respiratory complications, including atelectasis, compared to intravenous induction. This study aimed to evaluate the impact of inhalation versus intravenous anesthesia induction on atelectasis formation in pediatric patients, as assessed by lung ultrasound (LUS).
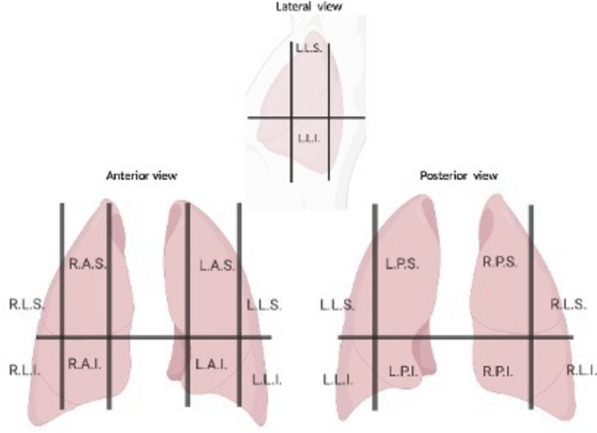
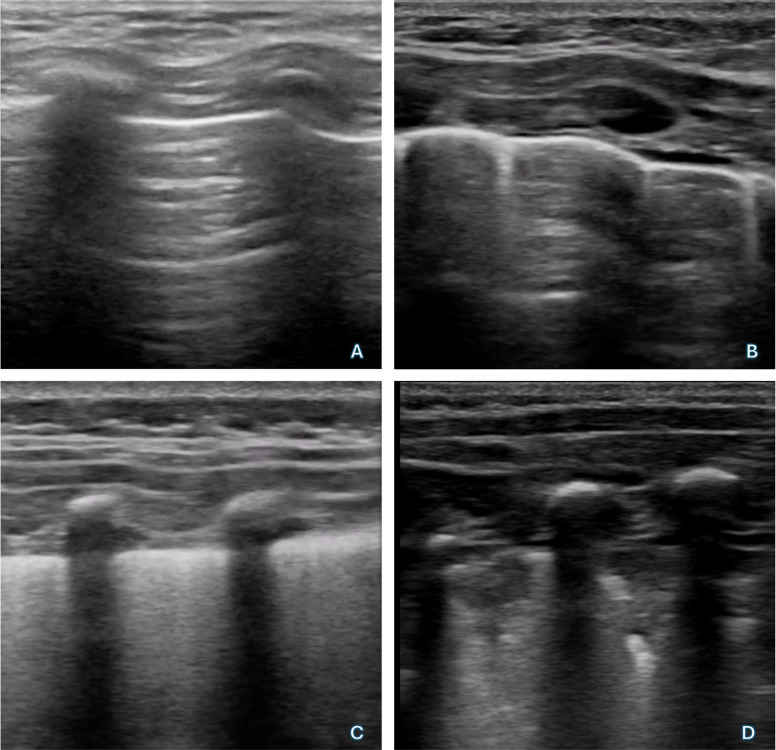
Methods: This propensity score-matched observational study was conducted at a tertiary pediatric hospital in Milan, Italy. Inclusion criteria were children ≤ 18 years undergoing elective surgery with general anesthesia. Patients were divided into inhalation and intravenous induction groups. LUS was performed before and after anesthesia induction to assess lung aeration. The primary endpoint was the global LUS score post-induction, with secondary endpoints including the incidence and distribution of atelectasis.
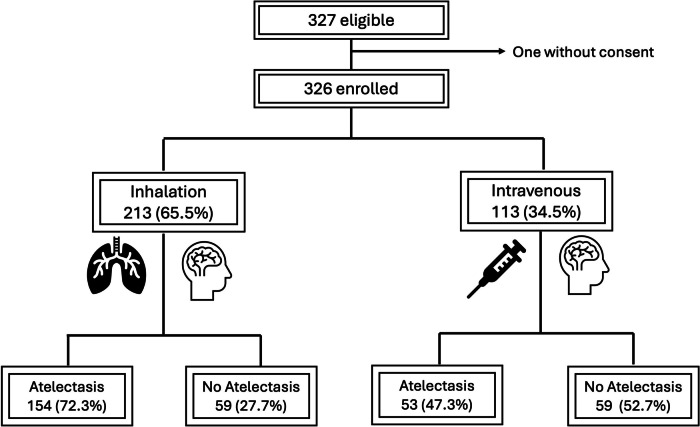
Results: Of the 326 patients included, 65% underwent inhalation induction and 35% intravenous induction. The global LUS score was significantly higher in the inhalation group (12.0 vs. 4.0, p < 0.001). After propensity score matching (for age, presence of upper respiratory tract infection, duration of induction, and PEEP levels at induction), average treatment effect (ATE) of mask induction was 5.89 (95% CI, 3.21-8.58; p < 0.001) point on LUS global score and a coefficient of 0.35 (OR 1.41) for atelectasis.
Discussion: Inhalation induction is associated with a higher incidence of atelectasis in pediatric patients also when we adjusted for clinically relevant covariates.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


