Lorenzo Torri, Petroula Nana, Giuseppe Panuccio, José Ignacio Torrealba, Daour Yousef El Sarhan, Tilo Kölbel
{"title":"用于慢性 B 型主动脉夹层选择性假腔排除的医生改良型漏斗状覆盖支架。","authors":"Lorenzo Torri, Petroula Nana, Giuseppe Panuccio, José Ignacio Torrealba, Daour Yousef El Sarhan, Tilo Kölbel","doi":"10.1177/17085381241289811","DOIUrl":null,"url":null,"abstract":"<p><p>PurposeTo describe the technique of off-centering a balloon-expandable covered stent for selective occlusion of a distal entry tear (ET) in a patient, conservatively treated for chronic type B aortic dissection (cTBAD), presenting FL expansion.TechniqueA 63-year-old male, with conservatively managed cTBAD, presented at follow-up with FL partial thrombosis and expansion (thoracic aorta FL from 21 mm to 27 mm and abdominal aorta FL from 11 mm to 15 mm in 6 months). No proximal ET was identifiable. Distal FL perfusion was caused by an ET in the abdominal aorta feeding a 2 mm accessory renal artery (ARA). As the aortic diameter was below the threshold for endovascular repair, a selective occlusion of the distal ET and ARA was planned. A balloon-expandable covered stent was modified by off-centering the covered stent proximally and resulting in a funnel-shape occluder after deployment across the ET into the ARA. To prevent type Ic endoleak due to possible FL expansion caused by an intra-operatively detected phrenic artery (PA), coils were deployed into the lumen of the modified stent and the ARA. The pre-discharge computed tomography angiography showed exclusion of both the ARA and ET and a type 2 endoleak from the PA.ConclusionA balloon-expandable covered stent can be modified by off-centering the covered stent resulting in a funnel shape to adapt to different diameter requirements.</p>","PeriodicalId":23549,"journal":{"name":"Vascular","volume":" ","pages":"1066-1073"},"PeriodicalIF":0.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450246/pdf/","citationCount":"0","resultStr":"{\"title\":\"Physician-modified funnel-shaped covered stent for selective false lumen exclusion in chronic type B aortic dissection.\",\"authors\":\"Lorenzo Torri, Petroula Nana, Giuseppe Panuccio, José Ignacio Torrealba, Daour Yousef El Sarhan, Tilo Kölbel\",\"doi\":\"10.1177/17085381241289811\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>PurposeTo describe the technique of off-centering a balloon-expandable covered stent for selective occlusion of a distal entry tear (ET) in a patient, conservatively treated for chronic type B aortic dissection (cTBAD), presenting FL expansion.TechniqueA 63-year-old male, with conservatively managed cTBAD, presented at follow-up with FL partial thrombosis and expansion (thoracic aorta FL from 21 mm to 27 mm and abdominal aorta FL from 11 mm to 15 mm in 6 months). No proximal ET was identifiable. Distal FL perfusion was caused by an ET in the abdominal aorta feeding a 2 mm accessory renal artery (ARA). As the aortic diameter was below the threshold for endovascular repair, a selective occlusion of the distal ET and ARA was planned. A balloon-expandable covered stent was modified by off-centering the covered stent proximally and resulting in a funnel-shape occluder after deployment across the ET into the ARA. To prevent type Ic endoleak due to possible FL expansion caused by an intra-operatively detected phrenic artery (PA), coils were deployed into the lumen of the modified stent and the ARA. The pre-discharge computed tomography angiography showed exclusion of both the ARA and ET and a type 2 endoleak from the PA.ConclusionA balloon-expandable covered stent can be modified by off-centering the covered stent resulting in a funnel shape to adapt to different diameter requirements.</p>\",\"PeriodicalId\":23549,\"journal\":{\"name\":\"Vascular\",\"volume\":\" \",\"pages\":\"1066-1073\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450246/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Vascular\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17085381241289811\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vascular","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17085381241289811","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/4 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
摘要
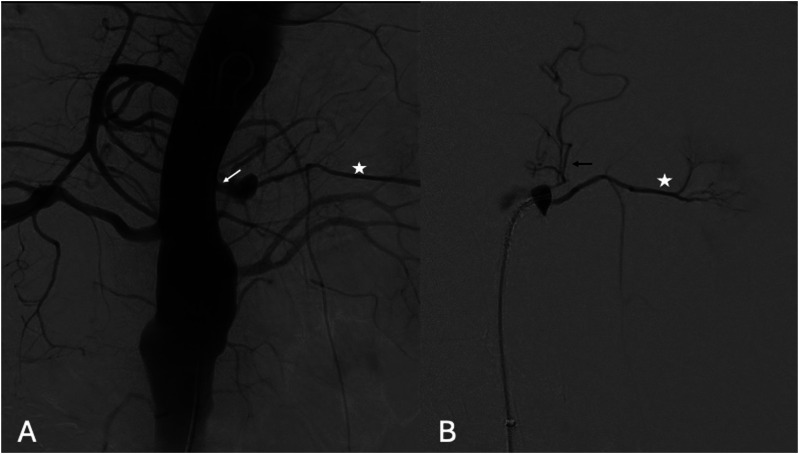
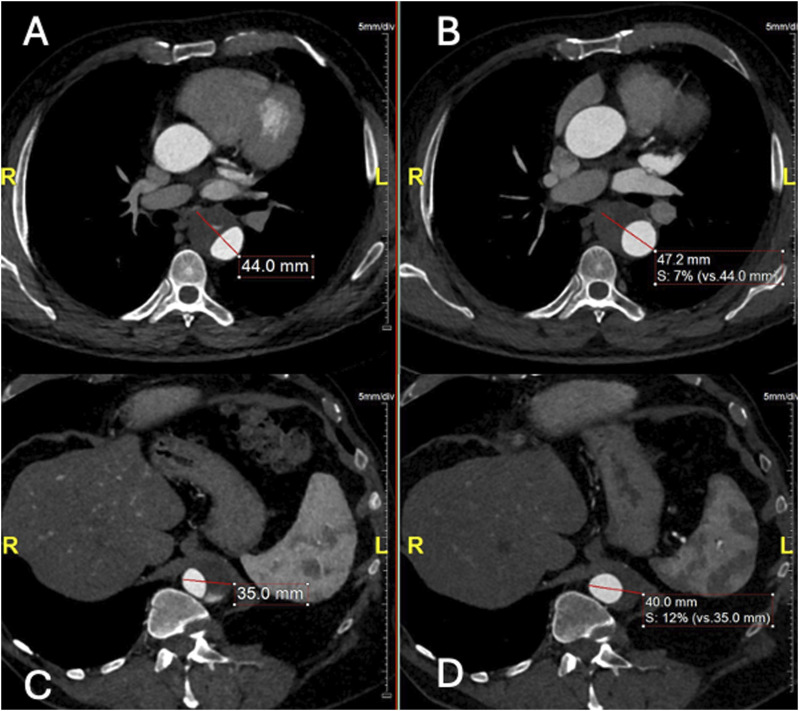
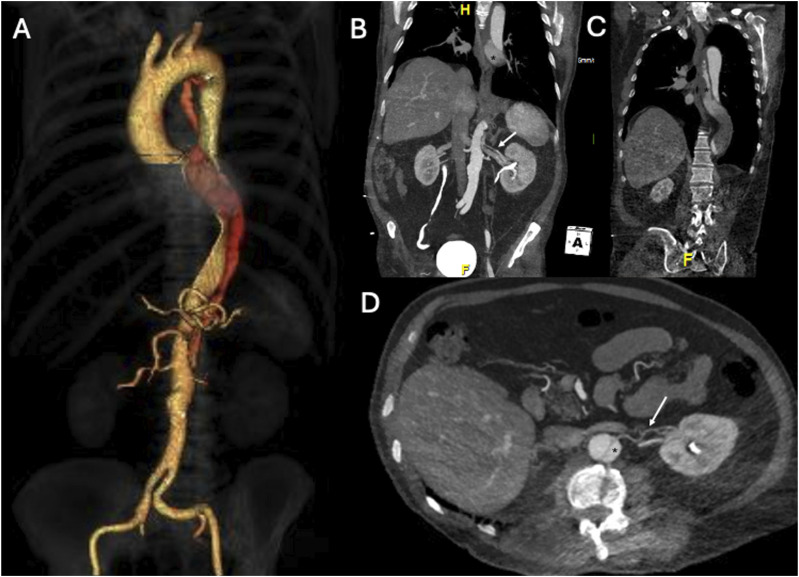
目的:描述在一名接受保守治疗的慢性 B 型主动脉夹层(cTBAD)患者中,采用偏离中心的球囊扩张覆盖支架选择性封堵远端入口撕裂(ET)的技术:一名 63 岁的男性,因慢性 B 型主动脉夹层(cTBAD)接受保守治疗,在随访时出现 FL 部分血栓形成和扩张(胸主动脉 FL 在 6 个月内从 21 mm 增至 27 mm,腹主动脉 FL 在 6 个月内从 11 mm 增至 15 mm)。未发现近端 ET。FL远端灌注是由腹主动脉中的ET造成的,ET为2毫米的肾脏附属动脉(ARA)供血。由于主动脉直径低于血管内修复的阈值,因此计划对远端 ET 和 ARA 进行选择性闭塞。对球囊扩张覆盖支架进行了改良,将覆盖支架向近端偏离中心,使其在穿过 ET 进入 ARA 后形成漏斗状闭塞。为防止术中检测到的膈动脉(PA)可能导致的FL扩张造成Ic型内漏,在改良支架和ARA的管腔内部署了线圈。出院前的计算机断层扫描血管造影显示,ARA和ET均被排除,PA出现了2型内漏:结论:球囊扩张型覆膜支架可通过偏离覆膜支架的中心形成漏斗状来进行改造,以适应不同直径的要求。
Physician-modified funnel-shaped covered stent for selective false lumen exclusion in chronic type B aortic dissection.
PurposeTo describe the technique of off-centering a balloon-expandable covered stent for selective occlusion of a distal entry tear (ET) in a patient, conservatively treated for chronic type B aortic dissection (cTBAD), presenting FL expansion.TechniqueA 63-year-old male, with conservatively managed cTBAD, presented at follow-up with FL partial thrombosis and expansion (thoracic aorta FL from 21 mm to 27 mm and abdominal aorta FL from 11 mm to 15 mm in 6 months). No proximal ET was identifiable. Distal FL perfusion was caused by an ET in the abdominal aorta feeding a 2 mm accessory renal artery (ARA). As the aortic diameter was below the threshold for endovascular repair, a selective occlusion of the distal ET and ARA was planned. A balloon-expandable covered stent was modified by off-centering the covered stent proximally and resulting in a funnel-shape occluder after deployment across the ET into the ARA. To prevent type Ic endoleak due to possible FL expansion caused by an intra-operatively detected phrenic artery (PA), coils were deployed into the lumen of the modified stent and the ARA. The pre-discharge computed tomography angiography showed exclusion of both the ARA and ET and a type 2 endoleak from the PA.ConclusionA balloon-expandable covered stent can be modified by off-centering the covered stent resulting in a funnel shape to adapt to different diameter requirements.
期刊介绍:
Vascular provides readers with new and unusual up-to-date articles and case reports focusing on vascular and endovascular topics. It is a highly international forum for the discussion and debate of all aspects of this distinct surgical specialty. It also features opinion pieces, literature reviews and controversial issues presented from various points of view.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


