下肢血管重建手术后手术部位感染相关结果的系统回顾和荟萃分析。
摘要
目的:虽然手术部位感染(SSI)是下肢血管重建手术后常用的质量指标,但与这种并发症相关的结果却很少被提及。我们对报告这些手术后发生 SSI 与临床结果和医疗资源使用之间关系的研究进行了系统回顾和荟萃分析:我们检索了 MEDLINE、Embase、CENTRAL 和循证医学综述(起始时间至 2023 年 4 月 4 日),以研究下肢血管重建手术后发生 SSI 与临床结果和医疗资源使用之间的调整关系。两名研究人员独立筛选摘要和全文引文、提取数据并评估偏倚风险。采用随机效应模型对数据进行汇总。使用 I2 统计量评估异质性。采用 GRADE 评估估计确定性:在确定的 6671 篇引文中,我们纳入了 11 项研究(n = 61628 名患者),这些研究报告了 SSI 的发生与 13 种不同结果之间的调整关联。发生 SSI 与再入院的调整风险增加(汇总调整风险比 (aRR) = 3.55;95% CI(置信区间)= 1.40-8.97;n = 4 项研究;n = 13,532 名患者;I2 = 99.0%;中等确定性)、30 天内旁路移植血栓形成(汇总 aRR = 2.09;95% CI = 1.41-3.09;n = 2 项研究;n = 23,240 名患者;I2 = 51.1%;低度确定性)、再次手术(汇总 aRR = 2.69;95% CI = 2.67-2.72;n = 2 项研究;n = 23 240 例患者;I2 = 0.0%;中度确定性)、需要输血或二次手术的出血(aRR = 1.40; 95% CI = 1.26-1.55; n = 1 项研究; n = 10,910 名患者; 低度确定性)、心肌梗死或中风(aRR = 1.21; 95% CI = 1.02-1.43; n = 1 项研究; n = 10,910 名患者; 低度确定性)和重大(即:踝关节以上)截肢(汇总 aRR = 1.93;95% CI = 1.26-2.95;n = 4 项研究;n = 32,859 例患者;I2 = 83.0;低确定性)。指数手术后 >30 天发生 SSI(aRR = 2.20;95% CI = 1.16-4.17;n = 3 项研究;n = 21,949 名患者;低确定性)和假体移植物感染(aRR = 6.72;95% CI = 3.21-12.70;n = 1 项研究;n = 272 名患者;低确定性)均与大截肢的调整后风险增加有关。假体移植物感染也与指数手术后30天以上的调整后死亡风险增加有关(aRR = 6.40; 95% CI = 3.32-12.36; n = 1项研究; n = 272例患者; 低确定性):本系统综述和荟萃分析表明,下肢血管重建手术后出现 SSI 会显著增加患者的发病率和医疗资源的使用。因此,SSI 是衡量此类手术质量的重要指标。然而,目前的估计是基于不同的、中低度确定性的证据,应该由大型、多中心、队列研究来证实。
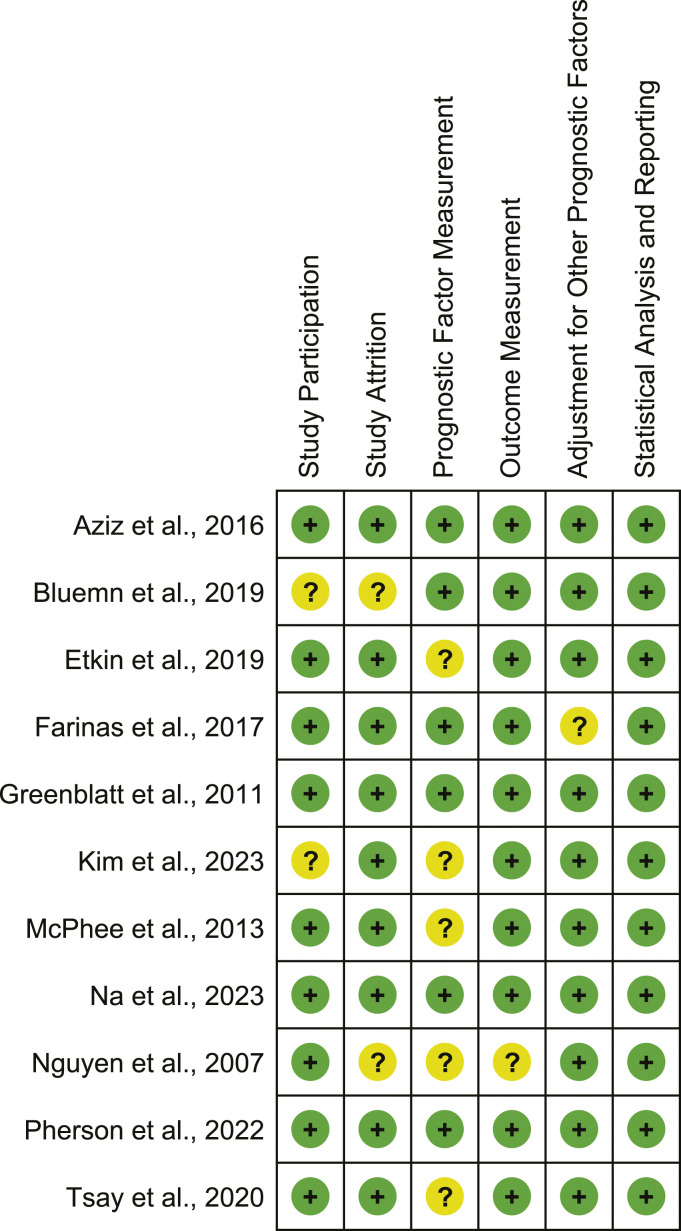
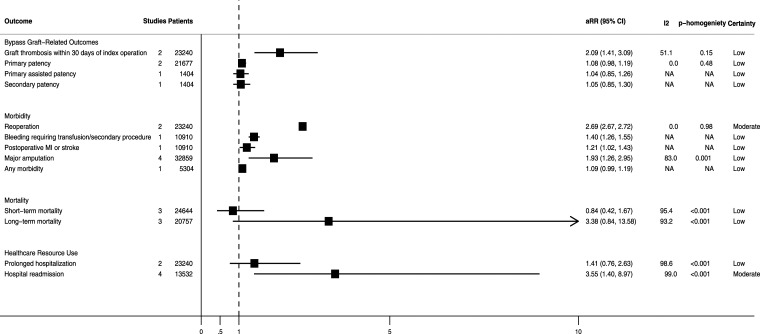
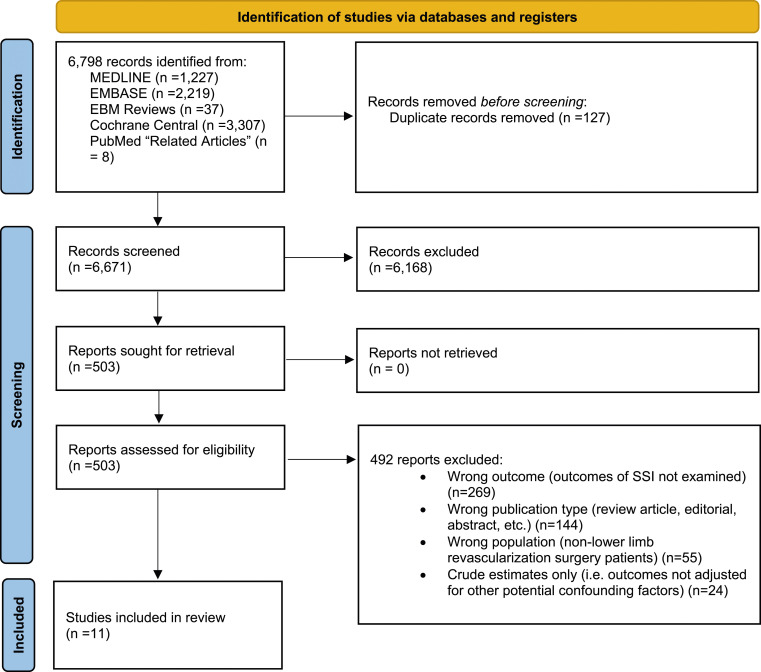
ObjectivesAlthough surgical site infection (SSI) is a commonly used quality metric after lower-limb revascularization surgery, outcomes associated with development of this complication are poorly characterized. We conducted a systematic review and meta-analysis of studies reporting associations between development of an SSI after these procedures and clinical outcomes and healthcare resource use.MethodsWe searched MEDLINE, Embase, CENTRAL, and Evidence-Based Medicine Reviews (inception to April 4th, 2023) for studies examining adjusted associations between development of an SSI after lower-limb revascularization surgery and clinical outcomes and healthcare resource use. Two investigators independently screened abstracts and full-text citations, extracted data, and assessed risk of bias. Data were pooled using random-effects models. Heterogeneity was assessed using I2 statistics. GRADE was used to assess estimate certainty.ResultsAmong 6671 citations identified, we included 11 studies (n = 61,628 total patients) that reported adjusted-associations between development of an SSI and 13 different outcomes. Developing an SSI was associated with an increased adjusted-risk of hospital readmission (pooled adjusted-risk ratio (aRR) = 3.55; 95% CI (confidence interval) = 1.40-8.97; n = 4 studies; n = 13,532 patients; I2 = 99.0%; moderate certainty), bypass graft thrombosis within 30-days (pooled aRR = 2.09; 95% CI = 1.41-3.09; n = 2 studies; n = 23,240 patients; I2 = 51.1%; low certainty), reoperation (pooled aRR = 2.69; 95% CI = 2.67-2.72; n = 2 studies; n = 23,240 patients; I2 = 0.0%; moderate certainty), bleeding requiring a transfusion or secondary procedure (aRR = 1.40; 95% CI = 1.26-1.55; n = 1 study; n = 10,910 patients; low certainty), myocardial infarction or stroke (aRR = 1.21; 95% CI = 1.02-1.43; n = 1 study; n = 10,910 patients; low certainty), and major (i.e., above-ankle) amputation (pooled aRR = 1.93; 95% CI = 1.26-2.95; n = 4 studies; n = 32,859 patients; I2 = 83.0; low certainty). Development of an SSI >30-days after the index operation (aRR = 2.20; 95% CI = 1.16-4.17; n = 3 studies; n = 21,949 patients; low certainty) and prosthetic graft infection (aRR = 6.72; 95% CI = 3.21-12.70; n = 1 study; n = 272 patients; low certainty) were both associated with an increased adjusted-risk of major amputation. Prosthetic graft infection was also associated with an increased adjusted-risk of mortality >30-days after the index procedure (aRR = 6.40; 95% CI = 3.32-12.36; n = 1 study; n = 272 patients; low certainty).ConclusionsThis systematic review and meta-analysis suggests that development of an SSI after lower-limb revascularization surgery significantly increases patient morbidity and healthcare resource use. SSI is therefore a valuable quality metric after these surgeries. However, current estimates are based on heterogenous, low-to-moderate certainty evidence and should be confirmed by large, multicenter, cohort studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


