Anthony Price, Christopher File, Alvin LeBlanc, Nathan Fredricks, Rylie Ju, Nathan Pratt, Rishi Lall, Daniel Jupiter
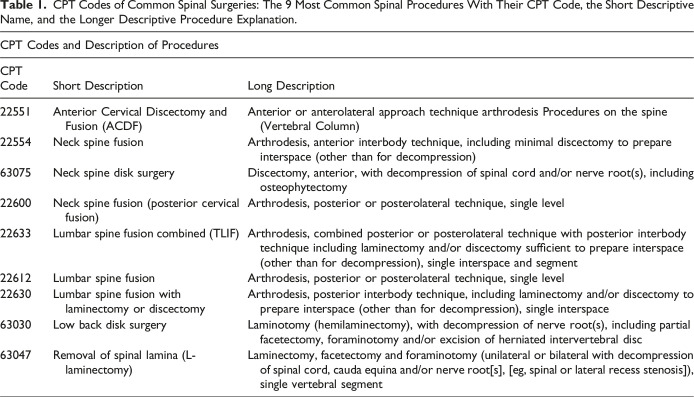
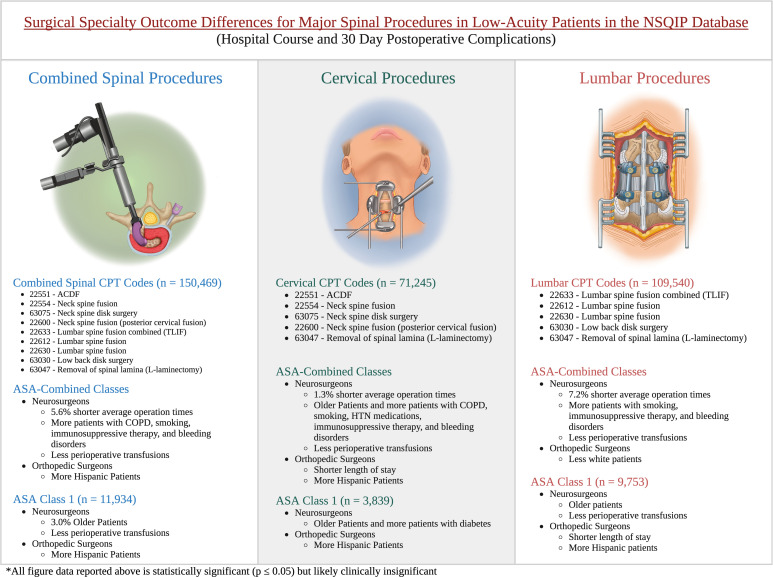
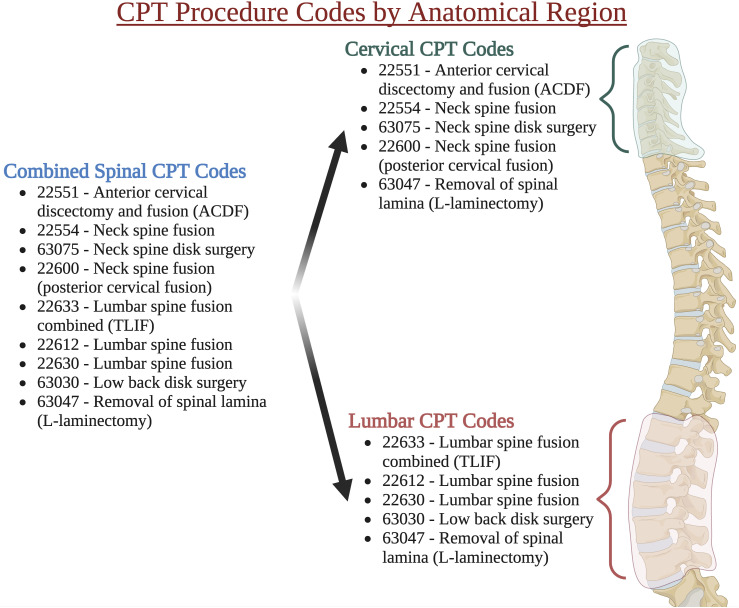
{"title":"低敏锐度患者主要脊柱手术的外科专科结果差异。","authors":"Anthony Price, Christopher File, Alvin LeBlanc, Nathan Fredricks, Rylie Ju, Nathan Pratt, Rishi Lall, Daniel Jupiter","doi":"10.1177/21925682241288500","DOIUrl":null,"url":null,"abstract":"<p><p>Study DesignRetrospective Cohort Study.ObjectivesThere is an ongoing debate as to the influence of specialty training on spine surgery. Alomari et al. indicated the influence of specialty on ACDF procedures. However, deeper analysis into other spine procedures and lower-acuity procedures has yet to occur. In this study, we aim to determine if the outcomes of the low American Society of Anesthesiologists (ASA) classification (ASA 1&2) patients undergoing spine surgery vary based on whether the operating surgeon was an orthopedic surgeon or a neurosurgeon.MethodsThe NSQIP databases from 2015 to 2021 were queried based on the CPT code for nine common spine procedures. Indicators of surgical course and successful outcomes were documented and compared between specialties.ResultsNeurosurgeons had minimally shorter operative times in the ASA 1&2 combined classification (ASA-C) group for cervical, lumbar, and combined spinal procedural groups. Neurosurgeons had a slightly lower percentage of perioperative transfusions in select ASA-C classes. Orthopedic surgeons had shorter lengths of stay for the cervical groups in ASA-C and ASA-1 classes (ASA-1). However, many specialty differences found in spine patients become less pronounced when considering only ASA-1 patients. Finally, postoperative complication outcomes and re-admission were similar between orthopedic and neurological surgeons in all cases.ConclusionsThese results, while statistically significant, are very likely clinically insignificant. They demonstrate that both orthopedic surgeons and neurosurgeons perform spinal surgery exceedingly safely with similarly low complication rates. This lays the groundwork for future exploration and benchmarking of performance in spine surgeries across neurosurgery and orthopedics.</p>","PeriodicalId":12680,"journal":{"name":"Global Spine Journal","volume":" ","pages":"2158-2168"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11559742/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Specialty Outcome Differences for Major Spinal Procedures in Low-Acuity Patients.\",\"authors\":\"Anthony Price, Christopher File, Alvin LeBlanc, Nathan Fredricks, Rylie Ju, Nathan Pratt, Rishi Lall, Daniel Jupiter\",\"doi\":\"10.1177/21925682241288500\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Study DesignRetrospective Cohort Study.ObjectivesThere is an ongoing debate as to the influence of specialty training on spine surgery. Alomari et al. indicated the influence of specialty on ACDF procedures. However, deeper analysis into other spine procedures and lower-acuity procedures has yet to occur. In this study, we aim to determine if the outcomes of the low American Society of Anesthesiologists (ASA) classification (ASA 1&2) patients undergoing spine surgery vary based on whether the operating surgeon was an orthopedic surgeon or a neurosurgeon.MethodsThe NSQIP databases from 2015 to 2021 were queried based on the CPT code for nine common spine procedures. Indicators of surgical course and successful outcomes were documented and compared between specialties.ResultsNeurosurgeons had minimally shorter operative times in the ASA 1&2 combined classification (ASA-C) group for cervical, lumbar, and combined spinal procedural groups. Neurosurgeons had a slightly lower percentage of perioperative transfusions in select ASA-C classes. Orthopedic surgeons had shorter lengths of stay for the cervical groups in ASA-C and ASA-1 classes (ASA-1). However, many specialty differences found in spine patients become less pronounced when considering only ASA-1 patients. Finally, postoperative complication outcomes and re-admission were similar between orthopedic and neurological surgeons in all cases.ConclusionsThese results, while statistically significant, are very likely clinically insignificant. They demonstrate that both orthopedic surgeons and neurosurgeons perform spinal surgery exceedingly safely with similarly low complication rates. This lays the groundwork for future exploration and benchmarking of performance in spine surgeries across neurosurgery and orthopedics.</p>\",\"PeriodicalId\":12680,\"journal\":{\"name\":\"Global Spine Journal\",\"volume\":\" \",\"pages\":\"2158-2168\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11559742/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Spine Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/21925682241288500\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Spine Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/21925682241288500","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Surgical Specialty Outcome Differences for Major Spinal Procedures in Low-Acuity Patients.
Study DesignRetrospective Cohort Study.ObjectivesThere is an ongoing debate as to the influence of specialty training on spine surgery. Alomari et al. indicated the influence of specialty on ACDF procedures. However, deeper analysis into other spine procedures and lower-acuity procedures has yet to occur. In this study, we aim to determine if the outcomes of the low American Society of Anesthesiologists (ASA) classification (ASA 1&2) patients undergoing spine surgery vary based on whether the operating surgeon was an orthopedic surgeon or a neurosurgeon.MethodsThe NSQIP databases from 2015 to 2021 were queried based on the CPT code for nine common spine procedures. Indicators of surgical course and successful outcomes were documented and compared between specialties.ResultsNeurosurgeons had minimally shorter operative times in the ASA 1&2 combined classification (ASA-C) group for cervical, lumbar, and combined spinal procedural groups. Neurosurgeons had a slightly lower percentage of perioperative transfusions in select ASA-C classes. Orthopedic surgeons had shorter lengths of stay for the cervical groups in ASA-C and ASA-1 classes (ASA-1). However, many specialty differences found in spine patients become less pronounced when considering only ASA-1 patients. Finally, postoperative complication outcomes and re-admission were similar between orthopedic and neurological surgeons in all cases.ConclusionsThese results, while statistically significant, are very likely clinically insignificant. They demonstrate that both orthopedic surgeons and neurosurgeons perform spinal surgery exceedingly safely with similarly low complication rates. This lays the groundwork for future exploration and benchmarking of performance in spine surgeries across neurosurgery and orthopedics.
期刊介绍:
Global Spine Journal (GSJ) is the official scientific publication of AOSpine. A peer-reviewed, open access journal, devoted to the study and treatment of spinal disorders, including diagnosis, operative and non-operative treatment options, surgical techniques, and emerging research and clinical developments.GSJ is indexed in PubMedCentral, SCOPUS, and Emerging Sources Citation Index (ESCI).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


