James A. Pasch MBBS, MSc, Hazel Serrao-Brown MD, ChD, MS, MPH, FRACS, Daniel Nguyen MBBS, MS, FRACS, Jaswinder S. Samra MBChB, DPhil (Oxon), FRCS (Eng&Ed), FRACS, Roderick Clifton-Bligh BSc (Med), MBBS (Hons), FRACP, PhD, FFSc (RCPA), Mark S. Sywak MBBS, MMed Sci (Clin Epi), FRACS
{"title":"外科医生在处理伴有心肌病的巨大出血性嗜铬细胞瘤时,耐心是关键。","authors":"James A. Pasch MBBS, MSc, Hazel Serrao-Brown MD, ChD, MS, MPH, FRACS, Daniel Nguyen MBBS, MS, FRACS, Jaswinder S. Samra MBChB, DPhil (Oxon), FRCS (Eng&Ed), FRACS, Roderick Clifton-Bligh BSc (Med), MBBS (Hons), FRACP, PhD, FFSc (RCPA), Mark S. Sywak MBBS, MMed Sci (Clin Epi), FRACS","doi":"10.1111/ans.19245","DOIUrl":null,"url":null,"abstract":"<p>A 26-year-old female presented with abdominal pain, hypertension and acute catecholamine cardiomyopathy secondary to a large phaeochromocytoma of the left adrenal gland. The patient had undiagnosed multiple endocrine neoplasia (MEN) 2A syndrome.</p><p>Following presentation, the patient was intubated due to reduced consciousness associated with labile blood pressure (60–200 mmHg systolic) and investigated with computed tomography (CT), which demonstrated a 125 mm solid/cystic left adrenal lesion with extracapsular haemorrhage (Fig. 1a). This was managed with angioembolisation of superior, middle and inferior arterial supply with coils and gelfoam slurry (Fig. 1b). CT also identified tumour thrombus extending into the left adrenal and renal veins. Following restoration of intravascular volume, alpha- and beta-blockade was commenced with phenoxybenzamine then metoprolol. The patient was extubated after 1 week with complete resolution of cardiac dysfunction after 3 weeks (initial LVEF <30%). Plasma metanephrine levels were elevated at 70 360 pmol/L (normal range: <660 pmol/L). Serum parathyroid hormone was also elevated at 16.9 pmol/L (1.6–6.9 pmol/L) and calcitonin 498 ng/L (<5 ng/L). A DOTATATE PET demonstrated peripheral rim avidity of the adrenal lesion with no uptake in the contralateral gland. A PET avid right thyroid nodule was confirmed as medullary thyroid carcinoma (MTC) on biopsy.</p><p>Following the resolution of cardiomyopathy, the tumour was excised by an open anterior approach. A midline laparotomy was performed with a Cattell-Braasch medial visceral rotation to access the aorta, inferior vena cava and proximal left renal vein. The lesser sac was entered, and the pancreas mobilized inferiorly to commence capsular dissection of the superomedial aspect of the tumour (Fig. 2a). The left renal vein was controlled, and tumour thrombus removed en bloc with the primary lesion via a longitudinal venotomy and primary repair with 6–0 prolene (Fig. 2b). The adrenal vein was ligated, and the tumour mobilized from the superior pole of kidney. The patient's recovery was complicated by a low-volume chyle leak managed successfully with drainage and low-fat diet. She is currently awaiting surgery for her MTC and primary hyperparathyroidism. Histopathology demonstrated a phaeochromocytoma without capsular invasion, Ki67 1%, mitotic count less than 1 per 2 mm<sup>2</sup> and retained staining for SDH-A and B mutations (Fig. 3b). Genetic testing confirmed a germline pathogenic variant in <i>RET</i> (634 codon) consistent with MEN2A.</p><p>Phaeochromocytoma crisis is a state of catecholamine excess, haemodynamic instability and end-organ dysfunction.<span><sup>1</sup></span> Even in such presentations, delay in surgery to allow optimisation of adrenergic blockade should be strongly pursued to avoid unacceptably high rates of mortality and morbidity.<span><sup>2</sup></span> Severe cardiogenic shock due to catecholamine cardiomyopathy is generally reversible with alpha-blockade, occasionally requiring adjuncts such as intra-aortic balloon pump and extracorporeal membrane oxygenation.<span><sup>2-4</sup></span> For patients with concomitant rupture, trans-arterial angioembolization is a successful strategy to gain haemodynamic control allowing time for alpha-blockade.<span><sup>5</sup></span> Care should also be taken in establishing the underlying cause of spontaneous adrenal haemorrhage considering alternate aetiologies such as other primary adrenal tumours or metastases as well as sepsis, coagulopathy and pregnancy.<span><sup>6</sup></span> This case demonstrates that the surgeon should exercise caution and patience in the acute management of phaeochromocytoma with multidisciplinary management in a specialized centre essential.</p><p>The patient has given informed consent for the publication of images.</p><p><b>James A. Pasch:</b> Writing – original draft. <b>Hazel Serrao-Brown:</b> Writing – review and editing. <b>Daniel Nguyen:</b> Supervision; writing – review and editing. <b>Jaswinder S. Samra:</b> Writing – review and editing. <b>Roderick Clifton-Bligh:</b> Writing – review and editing. <b>Mark S. Sywak:</b> Supervision; writing – review and editing.</p>","PeriodicalId":8158,"journal":{"name":"ANZ Journal of Surgery","volume":"94 11","pages":"2081-2083"},"PeriodicalIF":1.5000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ans.19245","citationCount":"0","resultStr":"{\"title\":\"Patience is key for the surgeon in the management of a large haemorrhagic phaeochromocytoma with cardiomyopathy\",\"authors\":\"James A. Pasch MBBS, MSc, Hazel Serrao-Brown MD, ChD, MS, MPH, FRACS, Daniel Nguyen MBBS, MS, FRACS, Jaswinder S. Samra MBChB, DPhil (Oxon), FRCS (Eng&Ed), FRACS, Roderick Clifton-Bligh BSc (Med), MBBS (Hons), FRACP, PhD, FFSc (RCPA), Mark S. Sywak MBBS, MMed Sci (Clin Epi), FRACS\",\"doi\":\"10.1111/ans.19245\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 26-year-old female presented with abdominal pain, hypertension and acute catecholamine cardiomyopathy secondary to a large phaeochromocytoma of the left adrenal gland. The patient had undiagnosed multiple endocrine neoplasia (MEN) 2A syndrome.</p><p>Following presentation, the patient was intubated due to reduced consciousness associated with labile blood pressure (60–200 mmHg systolic) and investigated with computed tomography (CT), which demonstrated a 125 mm solid/cystic left adrenal lesion with extracapsular haemorrhage (Fig. 1a). This was managed with angioembolisation of superior, middle and inferior arterial supply with coils and gelfoam slurry (Fig. 1b). CT also identified tumour thrombus extending into the left adrenal and renal veins. Following restoration of intravascular volume, alpha- and beta-blockade was commenced with phenoxybenzamine then metoprolol. The patient was extubated after 1 week with complete resolution of cardiac dysfunction after 3 weeks (initial LVEF <30%). Plasma metanephrine levels were elevated at 70 360 pmol/L (normal range: <660 pmol/L). Serum parathyroid hormone was also elevated at 16.9 pmol/L (1.6–6.9 pmol/L) and calcitonin 498 ng/L (<5 ng/L). A DOTATATE PET demonstrated peripheral rim avidity of the adrenal lesion with no uptake in the contralateral gland. A PET avid right thyroid nodule was confirmed as medullary thyroid carcinoma (MTC) on biopsy.</p><p>Following the resolution of cardiomyopathy, the tumour was excised by an open anterior approach. A midline laparotomy was performed with a Cattell-Braasch medial visceral rotation to access the aorta, inferior vena cava and proximal left renal vein. The lesser sac was entered, and the pancreas mobilized inferiorly to commence capsular dissection of the superomedial aspect of the tumour (Fig. 2a). The left renal vein was controlled, and tumour thrombus removed en bloc with the primary lesion via a longitudinal venotomy and primary repair with 6–0 prolene (Fig. 2b). The adrenal vein was ligated, and the tumour mobilized from the superior pole of kidney. The patient's recovery was complicated by a low-volume chyle leak managed successfully with drainage and low-fat diet. She is currently awaiting surgery for her MTC and primary hyperparathyroidism. Histopathology demonstrated a phaeochromocytoma without capsular invasion, Ki67 1%, mitotic count less than 1 per 2 mm<sup>2</sup> and retained staining for SDH-A and B mutations (Fig. 3b). Genetic testing confirmed a germline pathogenic variant in <i>RET</i> (634 codon) consistent with MEN2A.</p><p>Phaeochromocytoma crisis is a state of catecholamine excess, haemodynamic instability and end-organ dysfunction.<span><sup>1</sup></span> Even in such presentations, delay in surgery to allow optimisation of adrenergic blockade should be strongly pursued to avoid unacceptably high rates of mortality and morbidity.<span><sup>2</sup></span> Severe cardiogenic shock due to catecholamine cardiomyopathy is generally reversible with alpha-blockade, occasionally requiring adjuncts such as intra-aortic balloon pump and extracorporeal membrane oxygenation.<span><sup>2-4</sup></span> For patients with concomitant rupture, trans-arterial angioembolization is a successful strategy to gain haemodynamic control allowing time for alpha-blockade.<span><sup>5</sup></span> Care should also be taken in establishing the underlying cause of spontaneous adrenal haemorrhage considering alternate aetiologies such as other primary adrenal tumours or metastases as well as sepsis, coagulopathy and pregnancy.<span><sup>6</sup></span> This case demonstrates that the surgeon should exercise caution and patience in the acute management of phaeochromocytoma with multidisciplinary management in a specialized centre essential.</p><p>The patient has given informed consent for the publication of images.</p><p><b>James A. Pasch:</b> Writing – original draft. <b>Hazel Serrao-Brown:</b> Writing – review and editing. <b>Daniel Nguyen:</b> Supervision; writing – review and editing. <b>Jaswinder S. Samra:</b> Writing – review and editing. <b>Roderick Clifton-Bligh:</b> Writing – review and editing. <b>Mark S. Sywak:</b> Supervision; writing – review and editing.</p>\",\"PeriodicalId\":8158,\"journal\":{\"name\":\"ANZ Journal of Surgery\",\"volume\":\"94 11\",\"pages\":\"2081-2083\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ans.19245\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ANZ Journal of Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ans.19245\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ANZ Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ans.19245","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Patience is key for the surgeon in the management of a large haemorrhagic phaeochromocytoma with cardiomyopathy
A 26-year-old female presented with abdominal pain, hypertension and acute catecholamine cardiomyopathy secondary to a large phaeochromocytoma of the left adrenal gland. The patient had undiagnosed multiple endocrine neoplasia (MEN) 2A syndrome.
Following presentation, the patient was intubated due to reduced consciousness associated with labile blood pressure (60–200 mmHg systolic) and investigated with computed tomography (CT), which demonstrated a 125 mm solid/cystic left adrenal lesion with extracapsular haemorrhage (Fig. 1a). This was managed with angioembolisation of superior, middle and inferior arterial supply with coils and gelfoam slurry (Fig. 1b). CT also identified tumour thrombus extending into the left adrenal and renal veins. Following restoration of intravascular volume, alpha- and beta-blockade was commenced with phenoxybenzamine then metoprolol. The patient was extubated after 1 week with complete resolution of cardiac dysfunction after 3 weeks (initial LVEF <30%). Plasma metanephrine levels were elevated at 70 360 pmol/L (normal range: <660 pmol/L). Serum parathyroid hormone was also elevated at 16.9 pmol/L (1.6–6.9 pmol/L) and calcitonin 498 ng/L (<5 ng/L). A DOTATATE PET demonstrated peripheral rim avidity of the adrenal lesion with no uptake in the contralateral gland. A PET avid right thyroid nodule was confirmed as medullary thyroid carcinoma (MTC) on biopsy.
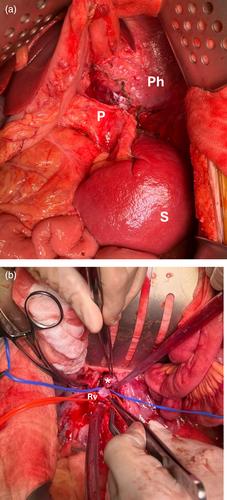
Following the resolution of cardiomyopathy, the tumour was excised by an open anterior approach. A midline laparotomy was performed with a Cattell-Braasch medial visceral rotation to access the aorta, inferior vena cava and proximal left renal vein. The lesser sac was entered, and the pancreas mobilized inferiorly to commence capsular dissection of the superomedial aspect of the tumour (Fig. 2a). The left renal vein was controlled, and tumour thrombus removed en bloc with the primary lesion via a longitudinal venotomy and primary repair with 6–0 prolene (Fig. 2b). The adrenal vein was ligated, and the tumour mobilized from the superior pole of kidney. The patient's recovery was complicated by a low-volume chyle leak managed successfully with drainage and low-fat diet. She is currently awaiting surgery for her MTC and primary hyperparathyroidism. Histopathology demonstrated a phaeochromocytoma without capsular invasion, Ki67 1%, mitotic count less than 1 per 2 mm2 and retained staining for SDH-A and B mutations (Fig. 3b). Genetic testing confirmed a germline pathogenic variant in RET (634 codon) consistent with MEN2A.
Phaeochromocytoma crisis is a state of catecholamine excess, haemodynamic instability and end-organ dysfunction.1 Even in such presentations, delay in surgery to allow optimisation of adrenergic blockade should be strongly pursued to avoid unacceptably high rates of mortality and morbidity.2 Severe cardiogenic shock due to catecholamine cardiomyopathy is generally reversible with alpha-blockade, occasionally requiring adjuncts such as intra-aortic balloon pump and extracorporeal membrane oxygenation.2-4 For patients with concomitant rupture, trans-arterial angioembolization is a successful strategy to gain haemodynamic control allowing time for alpha-blockade.5 Care should also be taken in establishing the underlying cause of spontaneous adrenal haemorrhage considering alternate aetiologies such as other primary adrenal tumours or metastases as well as sepsis, coagulopathy and pregnancy.6 This case demonstrates that the surgeon should exercise caution and patience in the acute management of phaeochromocytoma with multidisciplinary management in a specialized centre essential.
The patient has given informed consent for the publication of images.
James A. Pasch: Writing – original draft. Hazel Serrao-Brown: Writing – review and editing. Daniel Nguyen: Supervision; writing – review and editing. Jaswinder S. Samra: Writing – review and editing. Roderick Clifton-Bligh: Writing – review and editing. Mark S. Sywak: Supervision; writing – review and editing.
期刊介绍:
ANZ Journal of Surgery is published by Wiley on behalf of the Royal Australasian College of Surgeons to provide a medium for the publication of peer-reviewed original contributions related to clinical practice and/or research in all fields of surgery and related disciplines. It also provides a programme of continuing education for surgeons. All articles are peer-reviewed by at least two researchers expert in the field of the submitted paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


