{"title":"25 年前、50 年前和 75 年前。","authors":"Julian A. Smith MBMS, MSurgEd, FRACS","doi":"10.1111/ans.19244","DOIUrl":null,"url":null,"abstract":"<p><b>Norris B, Solomon MJ, Eyers AA, West RH, Glenn DC, Morgan BP. Abdominal surgery in the older Crohn's population. <i>ANZ. J. Surg</i>. 1999;69:199–204.</b></p><p>The surgical literature perceives that the elderly cohort of Crohn's patients may have increased risk with surgery. A retrospective review and prospective database analysis of all patients with histologically proven Crohn's disease who had a laparotomy at a single Sydney teaching hospital were performed. The last laparotomy of each patient was included in the analysis for morbidity and mortality to assess whether an older cohort was at an increased risk. A total of 156 patients had 298 laparotomies for histopathologically proven Crohn's disease. The frequency distribution of age at last laparotomy was bimodal, and the statistically determined cut-off age between younger and older cohorts was 55 years. Thirty-three patients were older than 55 years. There was no difference in duration of symptoms before first diagnosis (older, 17 months vs. younger, 25 months), previous number of Crohn's operations (42.4% vs. 39.8%), or duration of known Crohn's disease. Isolated large bowel disease was more common in the elderly cohort (42.4% vs. 18.7%, χ<sup>2</sup> = 8.09, <i>P</i> < 0.01). Small bowel and ileocaecal resections were more common in the younger cohort (72.4% vs. 51.6%, χ<sup>2</sup> = 5.19, <i>P</i> < 0.025). There was one death in each cohort (overall mortality 1.3%) and anastomotic leak rates (defined as the number of leaks per number of patients with anastomoses), were 4.3% (older) vs. 5.3% (younger) despite frank sepsis present in 21.2% of all subjects at the time of surgery. The older group had more cardiac (18.2% vs. 0.8%, <i>P</i> < 0.001) and respiratory complications (18.2% vs. 2.4%, <i>P</i> = 0.0003) and a longer mean but not median postoperative hospital admission. In conclusion, clinical features and presentation are similar in the older and younger Crohn's patients having a laparotomy. However, in the older patient there is a greater likelihood of large bowel disease, ileocaecal resection is done less commonly, there is a higher risk of minor cardiopulmonary postoperative complications, but with similar mortality and anastomotic leak rates to the younger patient.</p><p><b>Rieger N, Collopy B, Fink R, Mackay J, Woods R, Keck J. Total colectomy for Crohn's disease. <i>ANZ. J. Surg</i>. 1999;69:28–30.</b></p><p>Total colectomy for Crohn's disease of the colon may be restorative with ileorectal anastomosis or with an ileostomy and rectal stump. The present paper retrospectively audits the results of total colectomy and in particular assesses the number of patients who had a permanent ileostomy and whether this was related to disease in the rectum at the time of the original operation. A retrospective case note review was undertaken of patients operated upon between 1968 and 1994. Thirty-eight patients were identified (mean age 35 years; range 17–65 years). One patient died perioperatively from an anastomotic leak. Median follow-up for the remaining patients was 7 years (range 1–29 years). Ileorectal anastomosis was performed in 17 patients and total colectomy and ileostomy in 20 patients. Indications for surgery were failure of medical treatment (61%); toxic colitis (18%); abscess (8%); perforation (5%); large bowel obstruction (5%); and colovesical fistula (3%). Subsequent proctectomy (14 patients, 38%) was more likely with subtotal colectomy and ileostomy (nine patients, 45%) than ileorectal anastomosis (five patients, 29%). This was not statistically significant (<i>P</i> = 0.33). Additionally, seven patients had diversion of the rectum making 21 with an ileostomy (57%). Rectal involvement at the time of the original procedure significantly increased the likelihood of permanent ileostomy (<i>P</i> = 0.001). The presence of anal disease did not increase the prospect of ileostomy. One patient died with advanced adenocarcinoma in a defunctioned rectum. A permanent ileostomy after total colectomy for Crohn's disease is common and significantly more likely with rectal involvement.</p><p><b>Jamieson KG. Surgical lesions in head injuries: their relative incidence, mortality rates and trends. <i>ANZ. J. Surg</i>. 1974;44:241–50.</b></p><p>An analysis is presented of I,235 lesions requiring surgical treatment in 1045 patients drawn from a series of ~11 000 admitted to hospital with head injuries in an 11-year period. Subdural hematomas were by far the most common lesions, outnumbering extradural hematomas by over three to one. Depressed fractures were the next most frequent lesions, with intracerebral hematomas and other lesions much less common. Incidences, pathology, mechanisms and causes, presentation, and mortality rates are dissected, and some trends in type and severity of injury are discussed. It is clear that disciplined surgical endeavour can save many lives when a head injury is sustained. Regular review of results is basic to that maintenance of discipline essential to the achievement of low mortality rates, which should approximate the 10% of all cases of extradural hematoma here reported. It is equally apparent that many lesions are necessarily beyond all surgical help and amenable only to prevention. The trends toward more severe injury here reported increase the urgency for surgeons to become involved in the obligation of prevention of injury.</p><p><b>Jamieson KG, Yelland JDN, Merry GS. Haemangioblastomas of hindbrain: a report of 18 cases. <i>ANZ. J. Surg</i>. 1974;44:254–7.</b></p><p>Eighteen cases of hemangioblastoma of the hindbrain are reported, with reference to age and sex incidence, association with von Hippel's angiomatosis retinae and Lindau's syndrome, distribution of lesions, and clinical presentation. The outcome of surgical intervention is discussed, and a case of recurrent and multiple tumours is presented. Haemangioblastomas' of the hindbrain are uncommon lesions in any series of cerebral tumours, but have interesting features with respect to their association with von Hippel's angiomatosis retinae and Lindau's syndrome, an occasional familial incidence, and the production of an erythropoietic factor causing high levels of haemoglobin and erythrocythaemia. Cystic lesions in the cerebellar hemisphere are by far the most frequent manifestation of the condition, and these are readily removed, with a good general prognosis but with some risk of recurrence. On the other hand, lesions involving the brain stem and solid tumours may be encountered, and these have a much less favourable prognosis.</p><p><b>Gale C. The approach to the upper abdomen. <i>ANZ. J. Surg</i>. 1949;19:86–9.</b></p><p>Two incisions, oblique in direction and apparently not described previously, are suggested for the approach to the upper abdomen for the majority of upper abdominal operations (Fig 1). Each may be extended at its inner end to allow access to the other side of the abdomen, and at its outer end into the thorax to form the abdomino-thoracic incision of Humphreys. Compared to vertical incisions, the author considers that the access obtained is superior, closure is more readily performed and appears to be stronger, and post-operative discomfort is much less.</p>","PeriodicalId":8158,"journal":{"name":"ANZ Journal of Surgery","volume":"94 10","pages":"1683-1684"},"PeriodicalIF":1.5000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ans.19244","citationCount":"0","resultStr":"{\"title\":\"25, 50 and 75 years ago\",\"authors\":\"Julian A. Smith MBMS, MSurgEd, FRACS\",\"doi\":\"10.1111/ans.19244\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>Norris B, Solomon MJ, Eyers AA, West RH, Glenn DC, Morgan BP. Abdominal surgery in the older Crohn's population. <i>ANZ. J. Surg</i>. 1999;69:199–204.</b></p><p>The surgical literature perceives that the elderly cohort of Crohn's patients may have increased risk with surgery. A retrospective review and prospective database analysis of all patients with histologically proven Crohn's disease who had a laparotomy at a single Sydney teaching hospital were performed. The last laparotomy of each patient was included in the analysis for morbidity and mortality to assess whether an older cohort was at an increased risk. A total of 156 patients had 298 laparotomies for histopathologically proven Crohn's disease. The frequency distribution of age at last laparotomy was bimodal, and the statistically determined cut-off age between younger and older cohorts was 55 years. Thirty-three patients were older than 55 years. There was no difference in duration of symptoms before first diagnosis (older, 17 months vs. younger, 25 months), previous number of Crohn's operations (42.4% vs. 39.8%), or duration of known Crohn's disease. Isolated large bowel disease was more common in the elderly cohort (42.4% vs. 18.7%, χ<sup>2</sup> = 8.09, <i>P</i> < 0.01). Small bowel and ileocaecal resections were more common in the younger cohort (72.4% vs. 51.6%, χ<sup>2</sup> = 5.19, <i>P</i> < 0.025). There was one death in each cohort (overall mortality 1.3%) and anastomotic leak rates (defined as the number of leaks per number of patients with anastomoses), were 4.3% (older) vs. 5.3% (younger) despite frank sepsis present in 21.2% of all subjects at the time of surgery. The older group had more cardiac (18.2% vs. 0.8%, <i>P</i> < 0.001) and respiratory complications (18.2% vs. 2.4%, <i>P</i> = 0.0003) and a longer mean but not median postoperative hospital admission. In conclusion, clinical features and presentation are similar in the older and younger Crohn's patients having a laparotomy. However, in the older patient there is a greater likelihood of large bowel disease, ileocaecal resection is done less commonly, there is a higher risk of minor cardiopulmonary postoperative complications, but with similar mortality and anastomotic leak rates to the younger patient.</p><p><b>Rieger N, Collopy B, Fink R, Mackay J, Woods R, Keck J. Total colectomy for Crohn's disease. <i>ANZ. J. Surg</i>. 1999;69:28–30.</b></p><p>Total colectomy for Crohn's disease of the colon may be restorative with ileorectal anastomosis or with an ileostomy and rectal stump. The present paper retrospectively audits the results of total colectomy and in particular assesses the number of patients who had a permanent ileostomy and whether this was related to disease in the rectum at the time of the original operation. A retrospective case note review was undertaken of patients operated upon between 1968 and 1994. Thirty-eight patients were identified (mean age 35 years; range 17–65 years). One patient died perioperatively from an anastomotic leak. Median follow-up for the remaining patients was 7 years (range 1–29 years). Ileorectal anastomosis was performed in 17 patients and total colectomy and ileostomy in 20 patients. Indications for surgery were failure of medical treatment (61%); toxic colitis (18%); abscess (8%); perforation (5%); large bowel obstruction (5%); and colovesical fistula (3%). Subsequent proctectomy (14 patients, 38%) was more likely with subtotal colectomy and ileostomy (nine patients, 45%) than ileorectal anastomosis (five patients, 29%). This was not statistically significant (<i>P</i> = 0.33). Additionally, seven patients had diversion of the rectum making 21 with an ileostomy (57%). Rectal involvement at the time of the original procedure significantly increased the likelihood of permanent ileostomy (<i>P</i> = 0.001). The presence of anal disease did not increase the prospect of ileostomy. One patient died with advanced adenocarcinoma in a defunctioned rectum. A permanent ileostomy after total colectomy for Crohn's disease is common and significantly more likely with rectal involvement.</p><p><b>Jamieson KG. Surgical lesions in head injuries: their relative incidence, mortality rates and trends. <i>ANZ. J. Surg</i>. 1974;44:241–50.</b></p><p>An analysis is presented of I,235 lesions requiring surgical treatment in 1045 patients drawn from a series of ~11 000 admitted to hospital with head injuries in an 11-year period. Subdural hematomas were by far the most common lesions, outnumbering extradural hematomas by over three to one. Depressed fractures were the next most frequent lesions, with intracerebral hematomas and other lesions much less common. Incidences, pathology, mechanisms and causes, presentation, and mortality rates are dissected, and some trends in type and severity of injury are discussed. It is clear that disciplined surgical endeavour can save many lives when a head injury is sustained. Regular review of results is basic to that maintenance of discipline essential to the achievement of low mortality rates, which should approximate the 10% of all cases of extradural hematoma here reported. It is equally apparent that many lesions are necessarily beyond all surgical help and amenable only to prevention. The trends toward more severe injury here reported increase the urgency for surgeons to become involved in the obligation of prevention of injury.</p><p><b>Jamieson KG, Yelland JDN, Merry GS. Haemangioblastomas of hindbrain: a report of 18 cases. <i>ANZ. J. Surg</i>. 1974;44:254–7.</b></p><p>Eighteen cases of hemangioblastoma of the hindbrain are reported, with reference to age and sex incidence, association with von Hippel's angiomatosis retinae and Lindau's syndrome, distribution of lesions, and clinical presentation. The outcome of surgical intervention is discussed, and a case of recurrent and multiple tumours is presented. Haemangioblastomas' of the hindbrain are uncommon lesions in any series of cerebral tumours, but have interesting features with respect to their association with von Hippel's angiomatosis retinae and Lindau's syndrome, an occasional familial incidence, and the production of an erythropoietic factor causing high levels of haemoglobin and erythrocythaemia. Cystic lesions in the cerebellar hemisphere are by far the most frequent manifestation of the condition, and these are readily removed, with a good general prognosis but with some risk of recurrence. On the other hand, lesions involving the brain stem and solid tumours may be encountered, and these have a much less favourable prognosis.</p><p><b>Gale C. The approach to the upper abdomen. <i>ANZ. J. Surg</i>. 1949;19:86–9.</b></p><p>Two incisions, oblique in direction and apparently not described previously, are suggested for the approach to the upper abdomen for the majority of upper abdominal operations (Fig 1). Each may be extended at its inner end to allow access to the other side of the abdomen, and at its outer end into the thorax to form the abdomino-thoracic incision of Humphreys. Compared to vertical incisions, the author considers that the access obtained is superior, closure is more readily performed and appears to be stronger, and post-operative discomfort is much less.</p>\",\"PeriodicalId\":8158,\"journal\":{\"name\":\"ANZ Journal of Surgery\",\"volume\":\"94 10\",\"pages\":\"1683-1684\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ans.19244\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ANZ Journal of Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ans.19244\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ANZ Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ans.19244","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Norris B, Solomon MJ, Eyers AA, West RH, Glenn DC, Morgan BP. Abdominal surgery in the older Crohn's population. ANZ. J. Surg. 1999;69:199–204.
The surgical literature perceives that the elderly cohort of Crohn's patients may have increased risk with surgery. A retrospective review and prospective database analysis of all patients with histologically proven Crohn's disease who had a laparotomy at a single Sydney teaching hospital were performed. The last laparotomy of each patient was included in the analysis for morbidity and mortality to assess whether an older cohort was at an increased risk. A total of 156 patients had 298 laparotomies for histopathologically proven Crohn's disease. The frequency distribution of age at last laparotomy was bimodal, and the statistically determined cut-off age between younger and older cohorts was 55 years. Thirty-three patients were older than 55 years. There was no difference in duration of symptoms before first diagnosis (older, 17 months vs. younger, 25 months), previous number of Crohn's operations (42.4% vs. 39.8%), or duration of known Crohn's disease. Isolated large bowel disease was more common in the elderly cohort (42.4% vs. 18.7%, χ2 = 8.09, P < 0.01). Small bowel and ileocaecal resections were more common in the younger cohort (72.4% vs. 51.6%, χ2 = 5.19, P < 0.025). There was one death in each cohort (overall mortality 1.3%) and anastomotic leak rates (defined as the number of leaks per number of patients with anastomoses), were 4.3% (older) vs. 5.3% (younger) despite frank sepsis present in 21.2% of all subjects at the time of surgery. The older group had more cardiac (18.2% vs. 0.8%, P < 0.001) and respiratory complications (18.2% vs. 2.4%, P = 0.0003) and a longer mean but not median postoperative hospital admission. In conclusion, clinical features and presentation are similar in the older and younger Crohn's patients having a laparotomy. However, in the older patient there is a greater likelihood of large bowel disease, ileocaecal resection is done less commonly, there is a higher risk of minor cardiopulmonary postoperative complications, but with similar mortality and anastomotic leak rates to the younger patient.
Rieger N, Collopy B, Fink R, Mackay J, Woods R, Keck J. Total colectomy for Crohn's disease. ANZ. J. Surg. 1999;69:28–30.
Total colectomy for Crohn's disease of the colon may be restorative with ileorectal anastomosis or with an ileostomy and rectal stump. The present paper retrospectively audits the results of total colectomy and in particular assesses the number of patients who had a permanent ileostomy and whether this was related to disease in the rectum at the time of the original operation. A retrospective case note review was undertaken of patients operated upon between 1968 and 1994. Thirty-eight patients were identified (mean age 35 years; range 17–65 years). One patient died perioperatively from an anastomotic leak. Median follow-up for the remaining patients was 7 years (range 1–29 years). Ileorectal anastomosis was performed in 17 patients and total colectomy and ileostomy in 20 patients. Indications for surgery were failure of medical treatment (61%); toxic colitis (18%); abscess (8%); perforation (5%); large bowel obstruction (5%); and colovesical fistula (3%). Subsequent proctectomy (14 patients, 38%) was more likely with subtotal colectomy and ileostomy (nine patients, 45%) than ileorectal anastomosis (five patients, 29%). This was not statistically significant (P = 0.33). Additionally, seven patients had diversion of the rectum making 21 with an ileostomy (57%). Rectal involvement at the time of the original procedure significantly increased the likelihood of permanent ileostomy (P = 0.001). The presence of anal disease did not increase the prospect of ileostomy. One patient died with advanced adenocarcinoma in a defunctioned rectum. A permanent ileostomy after total colectomy for Crohn's disease is common and significantly more likely with rectal involvement.
Jamieson KG. Surgical lesions in head injuries: their relative incidence, mortality rates and trends. ANZ. J. Surg. 1974;44:241–50.
An analysis is presented of I,235 lesions requiring surgical treatment in 1045 patients drawn from a series of ~11 000 admitted to hospital with head injuries in an 11-year period. Subdural hematomas were by far the most common lesions, outnumbering extradural hematomas by over three to one. Depressed fractures were the next most frequent lesions, with intracerebral hematomas and other lesions much less common. Incidences, pathology, mechanisms and causes, presentation, and mortality rates are dissected, and some trends in type and severity of injury are discussed. It is clear that disciplined surgical endeavour can save many lives when a head injury is sustained. Regular review of results is basic to that maintenance of discipline essential to the achievement of low mortality rates, which should approximate the 10% of all cases of extradural hematoma here reported. It is equally apparent that many lesions are necessarily beyond all surgical help and amenable only to prevention. The trends toward more severe injury here reported increase the urgency for surgeons to become involved in the obligation of prevention of injury.
Jamieson KG, Yelland JDN, Merry GS. Haemangioblastomas of hindbrain: a report of 18 cases. ANZ. J. Surg. 1974;44:254–7.
Eighteen cases of hemangioblastoma of the hindbrain are reported, with reference to age and sex incidence, association with von Hippel's angiomatosis retinae and Lindau's syndrome, distribution of lesions, and clinical presentation. The outcome of surgical intervention is discussed, and a case of recurrent and multiple tumours is presented. Haemangioblastomas' of the hindbrain are uncommon lesions in any series of cerebral tumours, but have interesting features with respect to their association with von Hippel's angiomatosis retinae and Lindau's syndrome, an occasional familial incidence, and the production of an erythropoietic factor causing high levels of haemoglobin and erythrocythaemia. Cystic lesions in the cerebellar hemisphere are by far the most frequent manifestation of the condition, and these are readily removed, with a good general prognosis but with some risk of recurrence. On the other hand, lesions involving the brain stem and solid tumours may be encountered, and these have a much less favourable prognosis.
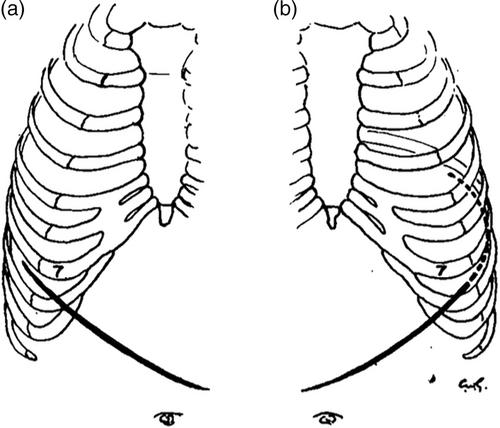
Gale C. The approach to the upper abdomen. ANZ. J. Surg. 1949;19:86–9.
Two incisions, oblique in direction and apparently not described previously, are suggested for the approach to the upper abdomen for the majority of upper abdominal operations (Fig 1). Each may be extended at its inner end to allow access to the other side of the abdomen, and at its outer end into the thorax to form the abdomino-thoracic incision of Humphreys. Compared to vertical incisions, the author considers that the access obtained is superior, closure is more readily performed and appears to be stronger, and post-operative discomfort is much less.
期刊介绍:
ANZ Journal of Surgery is published by Wiley on behalf of the Royal Australasian College of Surgeons to provide a medium for the publication of peer-reviewed original contributions related to clinical practice and/or research in all fields of surgery and related disciplines. It also provides a programme of continuing education for surgeons. All articles are peer-reviewed by at least two researchers expert in the field of the submitted paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


