{"title":"日本孕早期的临床挑战:妊娠糖尿病的最新进展。","authors":"Takashi Sugiyama, Maki Kawasaki, Naoko Arata","doi":"10.1111/jdi.14319","DOIUrl":null,"url":null,"abstract":"<p>The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study<span><sup>1</sup></span> and subsequently follow-up studies<span><sup>2-4</sup></span> have reported that gestational diabetes mellitus (GDM) is associated with various adverse pregnancy outcomes, which increases the mother's susceptibility to developing type 2 diabetes, and the child's susceptibility to developing obesity and impaired glucose tolerance in the future<span><sup>3-5</sup></span>.</p><p>GDM is diagnosed based on the presence of at least one of the following criteria: pre-load, 1- and 2-h values of the 75-g oral glucose tolerance test (75-g OGTT) of 92, 180 and 153 mg/dL, respectively, at 24–28 weeks' gestation<span><sup>6</sup></span>. These cutoff values were established and recommended by the International Association of Diabetes and Pregnancy Study Groups (IADPSG)<span><sup>6</sup></span>, based on the results of the HAPO study<span><sup>1</sup></span>.</p><p>The diagnostic criteria in Japan are the same as those of the IADPSG<span><sup>7</sup></span>. Although Japan did not participate in the HAPO study, a separate Japanese epidemiological study showed that GDM diagnosed during the second half of pregnancy using these diagnostic criteria was associated with a significantly higher risk of premature birth (<37 weeks), birthweight >90th percentile, hypertensive disorders of pregnancy and cesarean section<span><sup>8</sup></span>. These findings show that the perinatal prognosis of GDM in the second half of pregnancy, as defined by these diagnostic criteria, is poor among Japanese women. Furthermore, Japan uses similar diagnostic cutoff values as the GDM diagnostic criteria in the first half of pregnancy as in the second half of pregnancy. This policy has led to an increase in the incidence of GDM in Japan, as well as other countries<span><sup>8, 9</sup></span>. Incidentally, one study on the prognosis of GDM in the first half of pregnancy in Japan reported that women diagnosed with GDM during the first half of pregnancy had a higher incidence of pre-eclampsia and cesarean section<span><sup>10</sup></span>. We also previously showed that a GDM diagnosis in early pregnancy was associated with adverse pregnancy outcomes compared with a GDM diagnosis in late pregnancy using a previous diagnostic criteria in Japan<span><sup>11</sup></span>. Indeed, it should also be noted that Australia, USA and the UK do not apply these criteria for GDM during early pregnancy so far.</p><p>An important point is that the HAPO study, which formed the basis of the diagnostic criteria for GDM, was based on the 75-g OGTT from 24 to 32 weeks of pregnancy, and not on the blood glucose levels identified during 75-g OGTT in the first half of pregnancy. Indeed, our research has shown that blood glucose levels during 75-g OGTT differ between early and late pregnancy<span><sup>12</sup></span>. As such, the diagnostic criteria for GDM during early pregnancy based on epidemiological and clinical studies should be considered.</p><p>Although the diagnostic criteria for GDM differ, several randomized controlled trials (RCTs) have provided evidence of improved perinatal outcomes of GDM in the second half of pregnancy. One such example is the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial. In that RCT, 75-g OGTT was carried out between 24 and 34 weeks of pregnancy, with GDM defined as a preloading value of <140 mg/dL and a 2-h loading value between 140 and 198 mg/dL. In the GDM cases in ACHOIS, the intervention group had a significantly lower risk of neonatal complications than the non-intervention group<span><sup>13</sup></span>. However, that RCT study was not based on the IADPSG criteria for GDM. A retrospective cohort study showed that GDM based on IADPSG criteria was associated with improved pregnancy outcomes, although it increases the incidence of GDM<span><sup>14</sup></span>.</p><p>In contrast, one report showed the effectiveness of treatment for GDM in the first half of pregnancy. The Treatment of Booking GDM (TOBOGM) study was an RCT carried out at 17 hospitals enrolling women during their first half of pregnancy<span><sup>15</sup></span>. In that RCT, pregnant women with risk factors for GDM underwent a 75-g OGTT at 4–19 weeks of gestation. Consequently, early GDM was diagnosed in women who met any one of the following criteria (preload value ≥92 mg/dL, 1-h loading value ≥180 mg/dL, 2-h loading value ≥153 mg/dL). The TOBOGM study outcomes included adverse neonatal events, hypertensive disorders of pregnancy and neonatal lean body mass<span><sup>15</sup></span>. In individuals with GDM in the first half of pregnancy, the intervention group had a significantly reduced risk of adverse neonatal events compared with the control group. Furthermore, no statistically significant differences were observed between hypertensive disorders of pregnancy and neonatal lean body mass.</p><p>In the TOBOGM study, a subgroup analysis that classified first-half GDM with a 75-g OGTT value was carried out<span><sup>15</sup></span>. In the HAPO study, the odds ratio for infant birth weight >90th percentile, umbilical cord blood C-peptide >90th percentile and infant body fat mass >90th percentile was 1.75 for 75-g OGTT pre-loading values of 92 mg/dL, 1-h loading values of 180 mg/dL and 2-h loading values of 153 mg/dL. Furthermore, the respective values with odds ratios of 2.00 for 75-g OGTT were 95 mg/dL pre-loading, 191 mg/dL at 1-h and 162 mg/dL at 2-h. The investigators defined patients who met any one of the 95, 191 or 162 mg/dL limits as the high-threshold group, whereas patients who did not meet these values were classified as the low-threshold group, allowing a comparison study. When the outcome was birthweight, no significant association was found between the high-threshold group's intervention and the risk of large for gestational age or small for gestational age in infants. In contrast, the low-threshold group's intervention reduced the risk in large for gestational age infants, but increased the risk in small for gestational age infants. These differences are presumed to reflect infant malnutrition caused by the intervention. Furthermore, a secondary analysis of the TOBOGM study showed that adverse perinatal outcomes were increased with GDM diagnosed during the first half of pregnancy, despite treatment from 24 to 28 weeks' gestation, compared with GDM diagnosed during the second half of pregnancy<span><sup>16</sup></span>. This report suggests that GDM in early pregnancy should be treated. As aforementioned, the diagnostic criteria for GDM in the first half of pregnancy used in the TOBOGM study were the same as those used in Japan; as such, these findings could be considered useful. However, it should be noted that many of the women who were studied met the Japanese definition of obesity in the TOBOGM study.</p><p>The perinatal prognosis of GDM is poor, in both the second and first halves of pregnancy. Although there is evidence that intervention in GDM in the second half of pregnancy improves perinatal prognosis, there is little direct evidence for GDM strictly defined as pre-loading value ≥92 mg/dL, 1-h loading value ≥180 mg/dL and 2-h loading value ≥153 mg/dL; as such, further intervention studies are essential in Japan. One registry study termed the Diabetes and Pregnancy Outcome for Mother and Baby study is currently underway in Japan<span><sup>17</sup></span>, and further analysis results are awaited (Figure 1).</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: N/A.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>","PeriodicalId":51250,"journal":{"name":"Journal of Diabetes Investigation","volume":"15 12","pages":"1729-1731"},"PeriodicalIF":3.1000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.14319","citationCount":"0","resultStr":"{\"title\":\"Clinical challenges in early pregnancy in Japan: An update on gestational diabetes\",\"authors\":\"Takashi Sugiyama, Maki Kawasaki, Naoko Arata\",\"doi\":\"10.1111/jdi.14319\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study<span><sup>1</sup></span> and subsequently follow-up studies<span><sup>2-4</sup></span> have reported that gestational diabetes mellitus (GDM) is associated with various adverse pregnancy outcomes, which increases the mother's susceptibility to developing type 2 diabetes, and the child's susceptibility to developing obesity and impaired glucose tolerance in the future<span><sup>3-5</sup></span>.</p><p>GDM is diagnosed based on the presence of at least one of the following criteria: pre-load, 1- and 2-h values of the 75-g oral glucose tolerance test (75-g OGTT) of 92, 180 and 153 mg/dL, respectively, at 24–28 weeks' gestation<span><sup>6</sup></span>. These cutoff values were established and recommended by the International Association of Diabetes and Pregnancy Study Groups (IADPSG)<span><sup>6</sup></span>, based on the results of the HAPO study<span><sup>1</sup></span>.</p><p>The diagnostic criteria in Japan are the same as those of the IADPSG<span><sup>7</sup></span>. Although Japan did not participate in the HAPO study, a separate Japanese epidemiological study showed that GDM diagnosed during the second half of pregnancy using these diagnostic criteria was associated with a significantly higher risk of premature birth (<37 weeks), birthweight >90th percentile, hypertensive disorders of pregnancy and cesarean section<span><sup>8</sup></span>. These findings show that the perinatal prognosis of GDM in the second half of pregnancy, as defined by these diagnostic criteria, is poor among Japanese women. Furthermore, Japan uses similar diagnostic cutoff values as the GDM diagnostic criteria in the first half of pregnancy as in the second half of pregnancy. This policy has led to an increase in the incidence of GDM in Japan, as well as other countries<span><sup>8, 9</sup></span>. Incidentally, one study on the prognosis of GDM in the first half of pregnancy in Japan reported that women diagnosed with GDM during the first half of pregnancy had a higher incidence of pre-eclampsia and cesarean section<span><sup>10</sup></span>. We also previously showed that a GDM diagnosis in early pregnancy was associated with adverse pregnancy outcomes compared with a GDM diagnosis in late pregnancy using a previous diagnostic criteria in Japan<span><sup>11</sup></span>. Indeed, it should also be noted that Australia, USA and the UK do not apply these criteria for GDM during early pregnancy so far.</p><p>An important point is that the HAPO study, which formed the basis of the diagnostic criteria for GDM, was based on the 75-g OGTT from 24 to 32 weeks of pregnancy, and not on the blood glucose levels identified during 75-g OGTT in the first half of pregnancy. Indeed, our research has shown that blood glucose levels during 75-g OGTT differ between early and late pregnancy<span><sup>12</sup></span>. As such, the diagnostic criteria for GDM during early pregnancy based on epidemiological and clinical studies should be considered.</p><p>Although the diagnostic criteria for GDM differ, several randomized controlled trials (RCTs) have provided evidence of improved perinatal outcomes of GDM in the second half of pregnancy. One such example is the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial. In that RCT, 75-g OGTT was carried out between 24 and 34 weeks of pregnancy, with GDM defined as a preloading value of <140 mg/dL and a 2-h loading value between 140 and 198 mg/dL. In the GDM cases in ACHOIS, the intervention group had a significantly lower risk of neonatal complications than the non-intervention group<span><sup>13</sup></span>. However, that RCT study was not based on the IADPSG criteria for GDM. A retrospective cohort study showed that GDM based on IADPSG criteria was associated with improved pregnancy outcomes, although it increases the incidence of GDM<span><sup>14</sup></span>.</p><p>In contrast, one report showed the effectiveness of treatment for GDM in the first half of pregnancy. The Treatment of Booking GDM (TOBOGM) study was an RCT carried out at 17 hospitals enrolling women during their first half of pregnancy<span><sup>15</sup></span>. In that RCT, pregnant women with risk factors for GDM underwent a 75-g OGTT at 4–19 weeks of gestation. Consequently, early GDM was diagnosed in women who met any one of the following criteria (preload value ≥92 mg/dL, 1-h loading value ≥180 mg/dL, 2-h loading value ≥153 mg/dL). The TOBOGM study outcomes included adverse neonatal events, hypertensive disorders of pregnancy and neonatal lean body mass<span><sup>15</sup></span>. In individuals with GDM in the first half of pregnancy, the intervention group had a significantly reduced risk of adverse neonatal events compared with the control group. Furthermore, no statistically significant differences were observed between hypertensive disorders of pregnancy and neonatal lean body mass.</p><p>In the TOBOGM study, a subgroup analysis that classified first-half GDM with a 75-g OGTT value was carried out<span><sup>15</sup></span>. In the HAPO study, the odds ratio for infant birth weight >90th percentile, umbilical cord blood C-peptide >90th percentile and infant body fat mass >90th percentile was 1.75 for 75-g OGTT pre-loading values of 92 mg/dL, 1-h loading values of 180 mg/dL and 2-h loading values of 153 mg/dL. Furthermore, the respective values with odds ratios of 2.00 for 75-g OGTT were 95 mg/dL pre-loading, 191 mg/dL at 1-h and 162 mg/dL at 2-h. The investigators defined patients who met any one of the 95, 191 or 162 mg/dL limits as the high-threshold group, whereas patients who did not meet these values were classified as the low-threshold group, allowing a comparison study. When the outcome was birthweight, no significant association was found between the high-threshold group's intervention and the risk of large for gestational age or small for gestational age in infants. In contrast, the low-threshold group's intervention reduced the risk in large for gestational age infants, but increased the risk in small for gestational age infants. These differences are presumed to reflect infant malnutrition caused by the intervention. Furthermore, a secondary analysis of the TOBOGM study showed that adverse perinatal outcomes were increased with GDM diagnosed during the first half of pregnancy, despite treatment from 24 to 28 weeks' gestation, compared with GDM diagnosed during the second half of pregnancy<span><sup>16</sup></span>. This report suggests that GDM in early pregnancy should be treated. As aforementioned, the diagnostic criteria for GDM in the first half of pregnancy used in the TOBOGM study were the same as those used in Japan; as such, these findings could be considered useful. However, it should be noted that many of the women who were studied met the Japanese definition of obesity in the TOBOGM study.</p><p>The perinatal prognosis of GDM is poor, in both the second and first halves of pregnancy. Although there is evidence that intervention in GDM in the second half of pregnancy improves perinatal prognosis, there is little direct evidence for GDM strictly defined as pre-loading value ≥92 mg/dL, 1-h loading value ≥180 mg/dL and 2-h loading value ≥153 mg/dL; as such, further intervention studies are essential in Japan. One registry study termed the Diabetes and Pregnancy Outcome for Mother and Baby study is currently underway in Japan<span><sup>17</sup></span>, and further analysis results are awaited (Figure 1).</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: N/A.</p><p>Informed consent: N/A.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal studies: N/A.</p>\",\"PeriodicalId\":51250,\"journal\":{\"name\":\"Journal of Diabetes Investigation\",\"volume\":\"15 12\",\"pages\":\"1729-1731\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jdi.14319\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Diabetes Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jdi.14319\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Diabetes Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jdi.14319","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
高血糖和不良妊娠结局(HAPO)研究1和随后的随访研究2-4报道,妊娠期糖尿病(GDM)与多种不良妊娠结局相关,这增加了母亲患2型糖尿病的易感性,并增加了儿童未来患肥胖和糖耐量受损的易感性3-5。GDM的诊断基于以下标准中的至少一项:妊娠24-28周时,负荷前、1- h和2-h 75-g口服葡萄糖耐量试验(75-g OGTT)值分别为92、180和153 mg/dL 6。这些临界值是由国际糖尿病和妊娠研究小组协会(IADPSG)根据HAPO研究的结果建立和推荐的。日本的诊断标准与IADPSG7的诊断标准相同。虽然日本没有参与HAPO的研究,但另一项日本流行病学研究显示,使用这些诊断标准在妊娠后半期诊断的GDM与早产(37周)、出生体重第90个百分点、妊娠高血压疾病和剖宫产的风险显著升高相关8。这些发现表明,根据这些诊断标准,妊娠后半期GDM的围产期预后在日本妇女中较差。此外,日本在妊娠前半期和妊娠后半期使用了类似的诊断截止值作为GDM诊断标准。这一政策导致GDM在日本以及其他国家的发病率增加8,9。顺便提一下,日本一项关于妊娠前半期GDM预后的研究报告称,妊娠前半期诊断为GDM的妇女先兆子痫和剖宫产的发生率较高10。我们之前也发现,与使用日本先前诊断标准的妊娠晚期GDM诊断相比,妊娠早期GDM诊断与不良妊娠结局相关11。的确,值得注意的是,到目前为止,澳大利亚、美国和英国并没有将这些标准应用于妊娠早期的GDM。重要的一点是,HAPO研究,作为GDM诊断标准的基础,是基于妊娠24 - 32周的75 g OGTT,而不是基于妊娠前半期75 g OGTT期间确定的血糖水平。事实上,我们的研究表明,在75克OGTT期间,妊娠早期和晚期的血糖水平是不同的。因此,应考虑基于流行病学和临床研究的妊娠早期GDM的诊断标准。尽管GDM的诊断标准不同,但几项随机对照试验(RCTs)已经提供了证据,证明妊娠后半期GDM的围产期结局有所改善。其中一个例子是澳大利亚孕妇碳水化合物不耐受研究(ACHOIS)试验。在该RCT中,妊娠24 - 34周期间进行75 g OGTT, GDM定义为预负荷值为140 mg/dL, 2小时负荷值为140 - 198 mg/dL。在ACHOIS的GDM病例中,干预组新生儿并发症的风险明显低于非干预组13。然而,该RCT研究并不是基于GDM的IADPSG标准。一项回顾性队列研究显示,基于IADPSG标准的GDM与妊娠结局改善相关,尽管它增加了GDM14的发生率。相比之下,一份报告显示妊娠前半期治疗GDM的有效性。妊娠期妊娠糖尿病的治疗(TOBOGM)研究是一项在17家医院进行的随机对照试验,纳入了怀孕前半期的妇女。在该随机对照试验中,具有GDM危险因素的孕妇在妊娠4-19周时接受75 g OGTT治疗。因此,满足以下任何一项标准(负荷前值≥92 mg/dL, 1小时负荷值≥180 mg/dL, 2小时负荷值≥153 mg/dL)的女性可诊断为早期GDM。TOBOGM的研究结果包括新生儿不良事件、妊娠高血压疾病和新生儿瘦体重。在妊娠前半期患有GDM的个体中,干预组与对照组相比,新生儿不良事件的风险显著降低。此外,妊娠期高血压疾病与新生儿瘦体重之间无统计学差异。在TOBOGM研究中,进行了亚组分析,将前半期GDM分类为75 g OGTT值15。在HAPO研究中,75 g OGTT预负荷值为92 mg/dL, 1 h负荷值为180 mg/dL, 2 h负荷值为153 mg/dL,婴儿出生体重90百分位数、脐带血c肽90百分位数和婴儿体脂质量90百分位数的比值比为1.75。比值比为2。 75-g OGTT预载95 mg/dL, 1 h 191 mg/dL, 2 h 162 mg/dL。研究人员将达到95,191或162 mg/dL限制中的任何一个的患者定义为高阈值组,而未达到这些值的患者被归类为低阈值组,以便进行比较研究。当结果是出生体重时,高阈值组的干预与婴儿胎龄大或胎龄小的风险之间没有明显的关联。相比之下,低阈值组的干预降低了大胎龄婴儿的风险,但增加了小胎龄婴儿的风险。这些差异被认为反映了干预造成的婴儿营养不良。此外,TOBOGM研究的二次分析表明,与妊娠后半段诊断的GDM相比,妊娠前半期诊断的GDM的不良围产期结局增加,尽管在妊娠24至28周进行了治疗。本报告建议妊娠早期GDM应予以治疗。如上所述,TOBOGM研究中使用的妊娠前半期GDM的诊断标准与日本使用的标准相同;因此,这些发现可以被认为是有用的。然而,应该指出的是,在TOBOGM研究中,许多被研究的女性符合日本对肥胖的定义。GDM的围产期预后较差,在妊娠的后半期和前半期都是如此。虽然有证据表明妊娠后半期干预GDM可改善围产儿预后,但很少有直接证据表明GDM严格定义为预负荷值≥92 mg/dL、1 h负荷值≥180 mg/dL和2 h负荷值≥153 mg/dL;因此,在日本进行进一步的干预研究是必要的。一项名为“母婴糖尿病与妊娠结局研究”的注册研究目前正在日本进行,进一步的分析结果正在等待中(图1)。作者声明无利益冲突。研究方案的批准:无。知情同意:无。注册表及注册编号研究/试验:无。动物研究:无。
Clinical challenges in early pregnancy in Japan: An update on gestational diabetes
The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study1 and subsequently follow-up studies2-4 have reported that gestational diabetes mellitus (GDM) is associated with various adverse pregnancy outcomes, which increases the mother's susceptibility to developing type 2 diabetes, and the child's susceptibility to developing obesity and impaired glucose tolerance in the future3-5.
GDM is diagnosed based on the presence of at least one of the following criteria: pre-load, 1- and 2-h values of the 75-g oral glucose tolerance test (75-g OGTT) of 92, 180 and 153 mg/dL, respectively, at 24–28 weeks' gestation6. These cutoff values were established and recommended by the International Association of Diabetes and Pregnancy Study Groups (IADPSG)6, based on the results of the HAPO study1.
The diagnostic criteria in Japan are the same as those of the IADPSG7. Although Japan did not participate in the HAPO study, a separate Japanese epidemiological study showed that GDM diagnosed during the second half of pregnancy using these diagnostic criteria was associated with a significantly higher risk of premature birth (<37 weeks), birthweight >90th percentile, hypertensive disorders of pregnancy and cesarean section8. These findings show that the perinatal prognosis of GDM in the second half of pregnancy, as defined by these diagnostic criteria, is poor among Japanese women. Furthermore, Japan uses similar diagnostic cutoff values as the GDM diagnostic criteria in the first half of pregnancy as in the second half of pregnancy. This policy has led to an increase in the incidence of GDM in Japan, as well as other countries8, 9. Incidentally, one study on the prognosis of GDM in the first half of pregnancy in Japan reported that women diagnosed with GDM during the first half of pregnancy had a higher incidence of pre-eclampsia and cesarean section10. We also previously showed that a GDM diagnosis in early pregnancy was associated with adverse pregnancy outcomes compared with a GDM diagnosis in late pregnancy using a previous diagnostic criteria in Japan11. Indeed, it should also be noted that Australia, USA and the UK do not apply these criteria for GDM during early pregnancy so far.
An important point is that the HAPO study, which formed the basis of the diagnostic criteria for GDM, was based on the 75-g OGTT from 24 to 32 weeks of pregnancy, and not on the blood glucose levels identified during 75-g OGTT in the first half of pregnancy. Indeed, our research has shown that blood glucose levels during 75-g OGTT differ between early and late pregnancy12. As such, the diagnostic criteria for GDM during early pregnancy based on epidemiological and clinical studies should be considered.
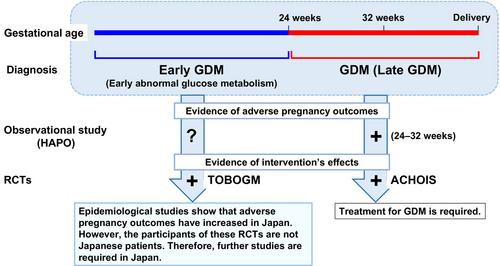
Although the diagnostic criteria for GDM differ, several randomized controlled trials (RCTs) have provided evidence of improved perinatal outcomes of GDM in the second half of pregnancy. One such example is the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial. In that RCT, 75-g OGTT was carried out between 24 and 34 weeks of pregnancy, with GDM defined as a preloading value of <140 mg/dL and a 2-h loading value between 140 and 198 mg/dL. In the GDM cases in ACHOIS, the intervention group had a significantly lower risk of neonatal complications than the non-intervention group13. However, that RCT study was not based on the IADPSG criteria for GDM. A retrospective cohort study showed that GDM based on IADPSG criteria was associated with improved pregnancy outcomes, although it increases the incidence of GDM14.
In contrast, one report showed the effectiveness of treatment for GDM in the first half of pregnancy. The Treatment of Booking GDM (TOBOGM) study was an RCT carried out at 17 hospitals enrolling women during their first half of pregnancy15. In that RCT, pregnant women with risk factors for GDM underwent a 75-g OGTT at 4–19 weeks of gestation. Consequently, early GDM was diagnosed in women who met any one of the following criteria (preload value ≥92 mg/dL, 1-h loading value ≥180 mg/dL, 2-h loading value ≥153 mg/dL). The TOBOGM study outcomes included adverse neonatal events, hypertensive disorders of pregnancy and neonatal lean body mass15. In individuals with GDM in the first half of pregnancy, the intervention group had a significantly reduced risk of adverse neonatal events compared with the control group. Furthermore, no statistically significant differences were observed between hypertensive disorders of pregnancy and neonatal lean body mass.
In the TOBOGM study, a subgroup analysis that classified first-half GDM with a 75-g OGTT value was carried out15. In the HAPO study, the odds ratio for infant birth weight >90th percentile, umbilical cord blood C-peptide >90th percentile and infant body fat mass >90th percentile was 1.75 for 75-g OGTT pre-loading values of 92 mg/dL, 1-h loading values of 180 mg/dL and 2-h loading values of 153 mg/dL. Furthermore, the respective values with odds ratios of 2.00 for 75-g OGTT were 95 mg/dL pre-loading, 191 mg/dL at 1-h and 162 mg/dL at 2-h. The investigators defined patients who met any one of the 95, 191 or 162 mg/dL limits as the high-threshold group, whereas patients who did not meet these values were classified as the low-threshold group, allowing a comparison study. When the outcome was birthweight, no significant association was found between the high-threshold group's intervention and the risk of large for gestational age or small for gestational age in infants. In contrast, the low-threshold group's intervention reduced the risk in large for gestational age infants, but increased the risk in small for gestational age infants. These differences are presumed to reflect infant malnutrition caused by the intervention. Furthermore, a secondary analysis of the TOBOGM study showed that adverse perinatal outcomes were increased with GDM diagnosed during the first half of pregnancy, despite treatment from 24 to 28 weeks' gestation, compared with GDM diagnosed during the second half of pregnancy16. This report suggests that GDM in early pregnancy should be treated. As aforementioned, the diagnostic criteria for GDM in the first half of pregnancy used in the TOBOGM study were the same as those used in Japan; as such, these findings could be considered useful. However, it should be noted that many of the women who were studied met the Japanese definition of obesity in the TOBOGM study.
The perinatal prognosis of GDM is poor, in both the second and first halves of pregnancy. Although there is evidence that intervention in GDM in the second half of pregnancy improves perinatal prognosis, there is little direct evidence for GDM strictly defined as pre-loading value ≥92 mg/dL, 1-h loading value ≥180 mg/dL and 2-h loading value ≥153 mg/dL; as such, further intervention studies are essential in Japan. One registry study termed the Diabetes and Pregnancy Outcome for Mother and Baby study is currently underway in Japan17, and further analysis results are awaited (Figure 1).
The authors declare no conflict of interest.
Approval of the research protocol: N/A.
Informed consent: N/A.
Registry and the registration no. of the study/trial: N/A.
期刊介绍:
Journal of Diabetes Investigation is your core diabetes journal from Asia; the official journal of the Asian Association for the Study of Diabetes (AASD). The journal publishes original research, country reports, commentaries, reviews, mini-reviews, case reports, letters, as well as editorials and news. Embracing clinical and experimental research in diabetes and related areas, the Journal of Diabetes Investigation includes aspects of prevention, treatment, as well as molecular aspects and pathophysiology. Translational research focused on the exchange of ideas between clinicians and researchers is also welcome. Journal of Diabetes Investigation is indexed by Science Citation Index Expanded (SCIE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


