{"title":"左旋多巴可能不足以抑制二氢蝶啶还原酶缺乏症患者泌乳素瘤的发展","authors":"Unai Diaz-Moreno, Cheng Guang Gan, Divya Pujari, Hoong-Wei Gan, Spyros Batzios","doi":"10.1210/jcemcr/luae172","DOIUrl":null,"url":null,"abstract":"<p><p>Dihydropteridine reductase (DHPR) deficiency is a disorder that prevents regeneration of tetrahydrobiopterin (BH4), causing hyperphenylalaninemia (HPA) and low levels of neurotransmitters, including dopamine. Due to low levels of dopamine, patients present with hyperprolactinemia. Treatment consists of a phenylalanine (Phe)-restricted diet, hydroxytryptophan and levodopa (L-Dopa) supplementation, leading to a rapid normalization of prolactin (PRL) levels. We report a case of a patient with DHPR deficiency presenting with new symptomatic hyperprolactinemia and amenorrhea in adolescence despite appropriate management. The prolactinoma was confirmed with pituitary magnetic resonance imaging. The patient was started on cabergoline with rapid normalization of PRL levels and resolution of symptoms, in keeping with previous reports. Cabergoline has a stronger affinity for the D2R receptor and longer half-life than L-Dopa, leading to lactotroph apoptosis, tumor shrinkage, and rapid and maintained normalization of PRL levels, with a better side-effect profile. Patients with DHPR deficiency need to be actively monitored for symptomatic hyperprolactinemia, as L-Dopa monotherapy is insufficient to suppress PRL secretion, leading to lactotroph hypertrophy and proliferation over time and development of prolactinomas in later life.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"2 10","pages":"luae172"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11427838/pdf/","citationCount":"0","resultStr":"{\"title\":\"L-Dopa Might Be Insufficient to Suppress Development of Prolactinomas in Dihydropteridine Reductase-Deficiency Patients.\",\"authors\":\"Unai Diaz-Moreno, Cheng Guang Gan, Divya Pujari, Hoong-Wei Gan, Spyros Batzios\",\"doi\":\"10.1210/jcemcr/luae172\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Dihydropteridine reductase (DHPR) deficiency is a disorder that prevents regeneration of tetrahydrobiopterin (BH4), causing hyperphenylalaninemia (HPA) and low levels of neurotransmitters, including dopamine. Due to low levels of dopamine, patients present with hyperprolactinemia. Treatment consists of a phenylalanine (Phe)-restricted diet, hydroxytryptophan and levodopa (L-Dopa) supplementation, leading to a rapid normalization of prolactin (PRL) levels. We report a case of a patient with DHPR deficiency presenting with new symptomatic hyperprolactinemia and amenorrhea in adolescence despite appropriate management. The prolactinoma was confirmed with pituitary magnetic resonance imaging. The patient was started on cabergoline with rapid normalization of PRL levels and resolution of symptoms, in keeping with previous reports. Cabergoline has a stronger affinity for the D2R receptor and longer half-life than L-Dopa, leading to lactotroph apoptosis, tumor shrinkage, and rapid and maintained normalization of PRL levels, with a better side-effect profile. Patients with DHPR deficiency need to be actively monitored for symptomatic hyperprolactinemia, as L-Dopa monotherapy is insufficient to suppress PRL secretion, leading to lactotroph hypertrophy and proliferation over time and development of prolactinomas in later life.</p>\",\"PeriodicalId\":73540,\"journal\":{\"name\":\"JCEM case reports\",\"volume\":\"2 10\",\"pages\":\"luae172\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11427838/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCEM case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1210/jcemcr/luae172\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luae172","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
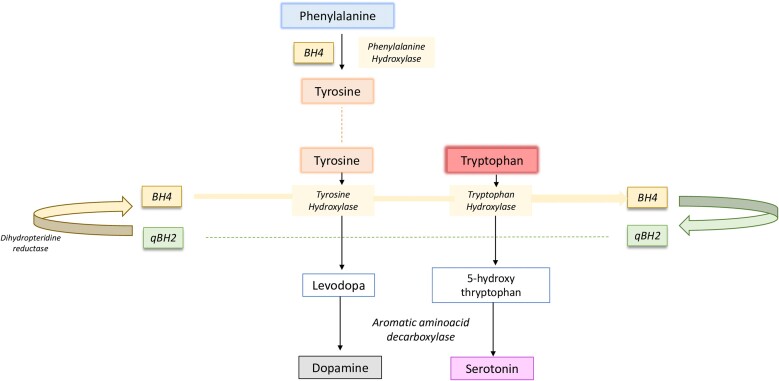
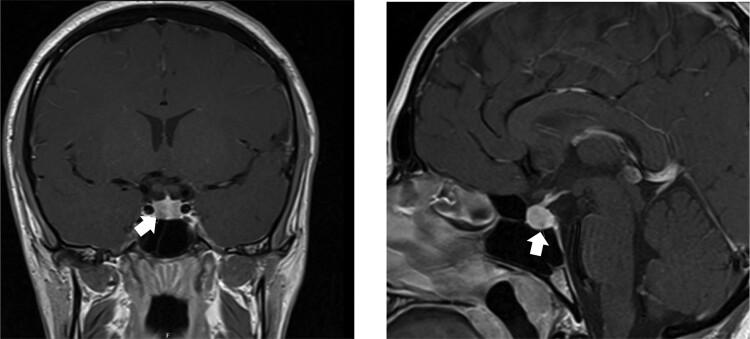
二氢蝶啶还原酶(DHPR)缺乏症是一种阻碍四氢生物蝶呤(BH4)再生的疾病,会导致高苯丙氨酸血症(HPA)和神经递质(包括多巴胺)水平低下。由于多巴胺水平低,患者会出现高泌乳素血症。治疗包括限制苯丙氨酸(Phe)饮食、补充羟色氨酸和左旋多巴(L-Dopa),从而使泌乳素(PRL)水平迅速恢复正常。我们报告了一例 DHPR 缺乏症患者的病例,尽管采取了适当的治疗措施,该患者仍在青春期出现了新的症状性高泌乳素血症和闭经。垂体磁共振成像确认了催乳素瘤。患者开始服用卡贝戈林,PRL 水平迅速恢复正常,症状也得到缓解,这与之前的报道一致。与左旋多巴相比,卡麦角林对D2R受体的亲和力更强,半衰期更长,可导致泌乳素凋亡、肿瘤缩小、PRL水平迅速恢复正常并保持不变,而且副作用更小。由于 L-Dopa 单一疗法不足以抑制 PRL 分泌,导致泌乳素细胞长期肥大和增殖,并在日后发展为催乳素瘤,因此需要积极监测 DHPR 缺乏症患者是否出现症状性高泌乳素血症。
L-Dopa Might Be Insufficient to Suppress Development of Prolactinomas in Dihydropteridine Reductase-Deficiency Patients.
Dihydropteridine reductase (DHPR) deficiency is a disorder that prevents regeneration of tetrahydrobiopterin (BH4), causing hyperphenylalaninemia (HPA) and low levels of neurotransmitters, including dopamine. Due to low levels of dopamine, patients present with hyperprolactinemia. Treatment consists of a phenylalanine (Phe)-restricted diet, hydroxytryptophan and levodopa (L-Dopa) supplementation, leading to a rapid normalization of prolactin (PRL) levels. We report a case of a patient with DHPR deficiency presenting with new symptomatic hyperprolactinemia and amenorrhea in adolescence despite appropriate management. The prolactinoma was confirmed with pituitary magnetic resonance imaging. The patient was started on cabergoline with rapid normalization of PRL levels and resolution of symptoms, in keeping with previous reports. Cabergoline has a stronger affinity for the D2R receptor and longer half-life than L-Dopa, leading to lactotroph apoptosis, tumor shrinkage, and rapid and maintained normalization of PRL levels, with a better side-effect profile. Patients with DHPR deficiency need to be actively monitored for symptomatic hyperprolactinemia, as L-Dopa monotherapy is insufficient to suppress PRL secretion, leading to lactotroph hypertrophy and proliferation over time and development of prolactinomas in later life.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


