Nathaniel J Williams, Nicholas C Cardamone, Rinad S Beidas, Steven C Marcus
{"title":"计算心理健康多层次实施试验的功率:有意义的效应大小、类内相关系数以及协变量解释的变异比例。","authors":"Nathaniel J Williams, Nicholas C Cardamone, Rinad S Beidas, Steven C Marcus","doi":"10.1177/26334895241279153","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite the ubiquity of multilevel sampling, design, and analysis in mental health implementation trials, few resources are available that provide reference values of design parameters (e.g., effect size, intraclass correlation coefficient [ICC], and proportion of variance explained by covariates [covariate <i>R</i> <sup>2</sup>]) needed to accurately determine sample size. The aim of this study was to provide empirical reference values for these parameters by aggregating data on implementation and clinical outcomes from multilevel implementation trials, including cluster randomized trials and individually randomized repeated measures trials, in mental health. The compendium of design parameters presented here represents plausible values that implementation scientists can use to guide sample size calculations for future trials.</p><p><strong>Method: </strong>We searched NIH RePORTER for all federally funded, multilevel implementation trials addressing mental health populations and settings from 2010 to 2020. For all continuous and binary implementation and clinical outcomes included in eligible trials, we generated values of effect size, ICC, and covariate <i>R<sup>2</sup></i> at each level via secondary analysis of trial data or via extraction of estimates from analyses in published research reports. Effect sizes were calculated as Cohen <i>d</i>; ICCs were generated via one-way random effects ANOVAs; covariate <i>R<sup>2</sup></i> estimates were calculated using the reduction in variance approach.</p><p><strong>Results: </strong>Seventeen trials were eligible, reporting on 53 implementation and clinical outcomes and 81 contrasts between implementation conditions. Tables of effect size, ICC, and covariate <i>R<sup>2</sup></i> are provided to guide implementation researchers in power analyses for designing multilevel implementation trials in mental health settings, including two- and three-level cluster randomized designs and unit-randomized repeated-measures designs.</p><p><strong>Conclusions: </strong>Researchers can use the empirical reference values reported in this study to develop meaningful sample size determinations for multilevel implementation trials in mental health. Discussion focuses on the application of the reference values reported in this study.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"5 ","pages":"26334895241279153"},"PeriodicalIF":2.6000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11437582/pdf/","citationCount":"0","resultStr":"{\"title\":\"Calculating power for multilevel implementation trials in mental health: Meaningful effect sizes, intraclass correlation coefficients, and proportions of variance explained by covariates.\",\"authors\":\"Nathaniel J Williams, Nicholas C Cardamone, Rinad S Beidas, Steven C Marcus\",\"doi\":\"10.1177/26334895241279153\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite the ubiquity of multilevel sampling, design, and analysis in mental health implementation trials, few resources are available that provide reference values of design parameters (e.g., effect size, intraclass correlation coefficient [ICC], and proportion of variance explained by covariates [covariate <i>R</i> <sup>2</sup>]) needed to accurately determine sample size. The aim of this study was to provide empirical reference values for these parameters by aggregating data on implementation and clinical outcomes from multilevel implementation trials, including cluster randomized trials and individually randomized repeated measures trials, in mental health. The compendium of design parameters presented here represents plausible values that implementation scientists can use to guide sample size calculations for future trials.</p><p><strong>Method: </strong>We searched NIH RePORTER for all federally funded, multilevel implementation trials addressing mental health populations and settings from 2010 to 2020. For all continuous and binary implementation and clinical outcomes included in eligible trials, we generated values of effect size, ICC, and covariate <i>R<sup>2</sup></i> at each level via secondary analysis of trial data or via extraction of estimates from analyses in published research reports. Effect sizes were calculated as Cohen <i>d</i>; ICCs were generated via one-way random effects ANOVAs; covariate <i>R<sup>2</sup></i> estimates were calculated using the reduction in variance approach.</p><p><strong>Results: </strong>Seventeen trials were eligible, reporting on 53 implementation and clinical outcomes and 81 contrasts between implementation conditions. Tables of effect size, ICC, and covariate <i>R<sup>2</sup></i> are provided to guide implementation researchers in power analyses for designing multilevel implementation trials in mental health settings, including two- and three-level cluster randomized designs and unit-randomized repeated-measures designs.</p><p><strong>Conclusions: </strong>Researchers can use the empirical reference values reported in this study to develop meaningful sample size determinations for multilevel implementation trials in mental health. Discussion focuses on the application of the reference values reported in this study.</p>\",\"PeriodicalId\":73354,\"journal\":{\"name\":\"Implementation research and practice\",\"volume\":\"5 \",\"pages\":\"26334895241279153\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11437582/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Implementation research and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/26334895241279153\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895241279153","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Calculating power for multilevel implementation trials in mental health: Meaningful effect sizes, intraclass correlation coefficients, and proportions of variance explained by covariates.
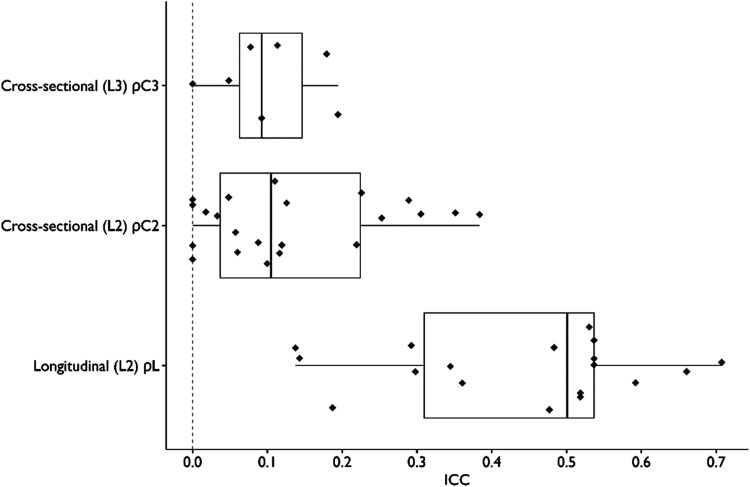
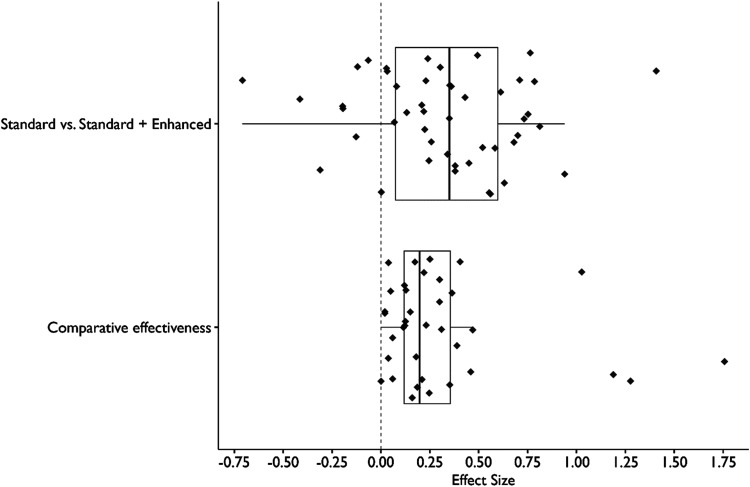
Background: Despite the ubiquity of multilevel sampling, design, and analysis in mental health implementation trials, few resources are available that provide reference values of design parameters (e.g., effect size, intraclass correlation coefficient [ICC], and proportion of variance explained by covariates [covariate R2]) needed to accurately determine sample size. The aim of this study was to provide empirical reference values for these parameters by aggregating data on implementation and clinical outcomes from multilevel implementation trials, including cluster randomized trials and individually randomized repeated measures trials, in mental health. The compendium of design parameters presented here represents plausible values that implementation scientists can use to guide sample size calculations for future trials.
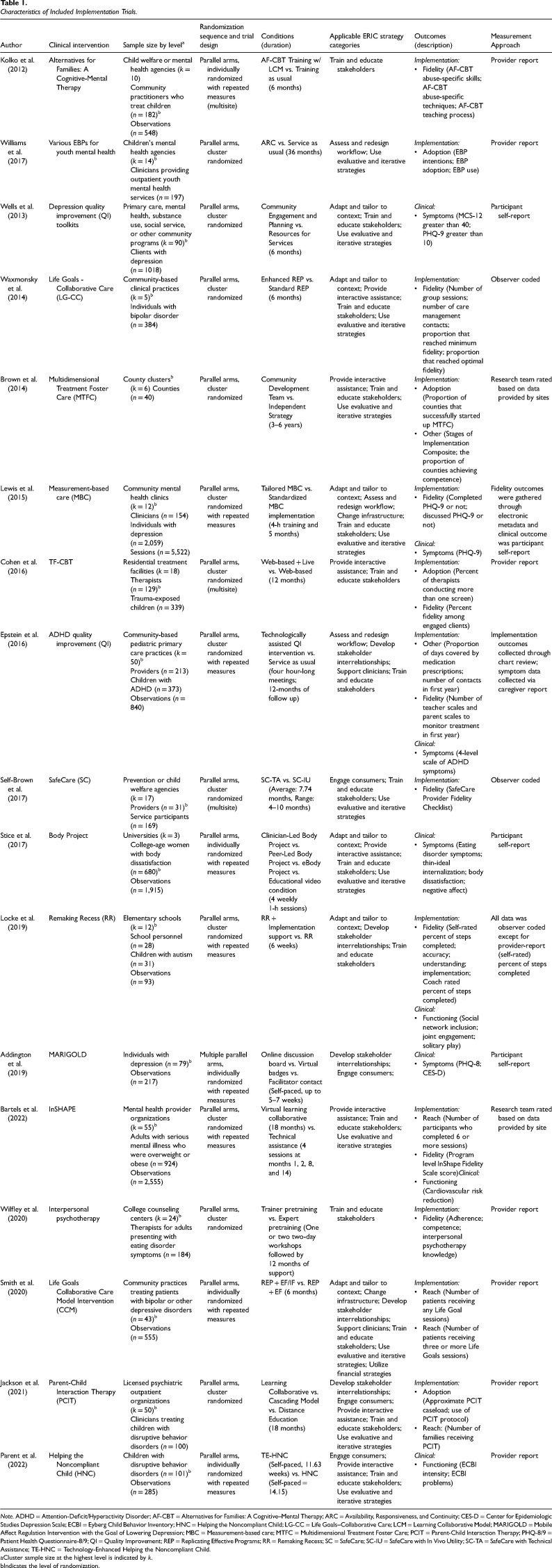
Method: We searched NIH RePORTER for all federally funded, multilevel implementation trials addressing mental health populations and settings from 2010 to 2020. For all continuous and binary implementation and clinical outcomes included in eligible trials, we generated values of effect size, ICC, and covariate R2 at each level via secondary analysis of trial data or via extraction of estimates from analyses in published research reports. Effect sizes were calculated as Cohen d; ICCs were generated via one-way random effects ANOVAs; covariate R2 estimates were calculated using the reduction in variance approach.
Results: Seventeen trials were eligible, reporting on 53 implementation and clinical outcomes and 81 contrasts between implementation conditions. Tables of effect size, ICC, and covariate R2 are provided to guide implementation researchers in power analyses for designing multilevel implementation trials in mental health settings, including two- and three-level cluster randomized designs and unit-randomized repeated-measures designs.
Conclusions: Researchers can use the empirical reference values reported in this study to develop meaningful sample size determinations for multilevel implementation trials in mental health. Discussion focuses on the application of the reference values reported in this study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


