Ruaraidh A. S. Campbell, Tharusan Thevathasan, Danny J. N. Wong, Andrew M. Wilson, Helen A. Lindsay, Douglas Campbell, Scott Popham, Lisa M. Barneto, Paul S. Myles, S. Ramani Moonesinghe, SNAP-2: EPICCS collaborators, Steve K. Harris
{"title":"重症监护病房床位供应与术后效果:一项多国队列研究","authors":"Ruaraidh A. S. Campbell, Tharusan Thevathasan, Danny J. N. Wong, Andrew M. Wilson, Helen A. Lindsay, Douglas Campbell, Scott Popham, Lisa M. Barneto, Paul S. Myles, S. Ramani Moonesinghe, SNAP-2: EPICCS collaborators, Steve K. Harris","doi":"10.1111/anae.16383","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Critical care beds are a limited resource, yet research indicates that recommendations for postoperative critical care admission based on patient-level risk stratification are not followed. It is unclear how prioritisation decisions are made in real-world settings and the effect of this prioritisation on outcomes.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a prespecified analysis of an observational cohort study of adult patients undergoing inpatient surgery, conducted in 274 hospitals across the UK and Australasia during 2017. The primary outcome was postoperative morbidity at day 7. Logistic regression models were used to evaluate the relationship between critical care admission and patient and health system factors. The causal effect of critical care admission on outcome was estimated using variation in critical care occupancy as a natural experiment in an instrumental variable analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 19,491 patients from 248 hospitals were eligible for analysis, of whom 2107 were directly admitted to critical care postoperatively. Postoperative morbidity occurred in 2829/19,491 (15%) patients. Increasing surgical risk was associated with critical care admission, as was increased availability of critical care beds (odds ratio (95%CI) 1.04 (1.01–1.06), p = 0.002) per available bed; however, the probability of admission varied significantly between hospitals (median odds ratio 3.05). There was no evidence of a difference in postoperative morbidity with critical care admission (odds ratio (95%CI) 0.91 (0.57–1.45), p = 0.710).</p>\n </section>\n \n <section>\n \n <h3> Discussion</h3>\n \n <p>Postoperative critical care admission is variable and related to bed availability. Statistical methods that adjust for unobserved confounding lowered the estimates of harm previously reported to have been associated with postoperative critical care admission. Our findings provide a rationale for a clinical trial which would evaluate any potential benefits for postoperative critical care admission for patients in whom there is no absolute indication for admission.</p>\n </section>\n </div>","PeriodicalId":7742,"journal":{"name":"Anaesthesia","volume":"79 11","pages":"1165-1179"},"PeriodicalIF":7.5000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16383","citationCount":"0","resultStr":"{\"title\":\"Critical care unit bed availability and postoperative outcomes: a multinational cohort study\",\"authors\":\"Ruaraidh A. S. Campbell, Tharusan Thevathasan, Danny J. N. Wong, Andrew M. Wilson, Helen A. Lindsay, Douglas Campbell, Scott Popham, Lisa M. Barneto, Paul S. Myles, S. Ramani Moonesinghe, SNAP-2: EPICCS collaborators, Steve K. Harris\",\"doi\":\"10.1111/anae.16383\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Critical care beds are a limited resource, yet research indicates that recommendations for postoperative critical care admission based on patient-level risk stratification are not followed. It is unclear how prioritisation decisions are made in real-world settings and the effect of this prioritisation on outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a prespecified analysis of an observational cohort study of adult patients undergoing inpatient surgery, conducted in 274 hospitals across the UK and Australasia during 2017. The primary outcome was postoperative morbidity at day 7. Logistic regression models were used to evaluate the relationship between critical care admission and patient and health system factors. The causal effect of critical care admission on outcome was estimated using variation in critical care occupancy as a natural experiment in an instrumental variable analysis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>A total of 19,491 patients from 248 hospitals were eligible for analysis, of whom 2107 were directly admitted to critical care postoperatively. Postoperative morbidity occurred in 2829/19,491 (15%) patients. Increasing surgical risk was associated with critical care admission, as was increased availability of critical care beds (odds ratio (95%CI) 1.04 (1.01–1.06), p = 0.002) per available bed; however, the probability of admission varied significantly between hospitals (median odds ratio 3.05). There was no evidence of a difference in postoperative morbidity with critical care admission (odds ratio (95%CI) 0.91 (0.57–1.45), p = 0.710).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Discussion</h3>\\n \\n <p>Postoperative critical care admission is variable and related to bed availability. Statistical methods that adjust for unobserved confounding lowered the estimates of harm previously reported to have been associated with postoperative critical care admission. Our findings provide a rationale for a clinical trial which would evaluate any potential benefits for postoperative critical care admission for patients in whom there is no absolute indication for admission.</p>\\n </section>\\n </div>\",\"PeriodicalId\":7742,\"journal\":{\"name\":\"Anaesthesia\",\"volume\":\"79 11\",\"pages\":\"1165-1179\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2024-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16383\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anaesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/anae.16383\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/anae.16383","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Critical care unit bed availability and postoperative outcomes: a multinational cohort study
Background
Critical care beds are a limited resource, yet research indicates that recommendations for postoperative critical care admission based on patient-level risk stratification are not followed. It is unclear how prioritisation decisions are made in real-world settings and the effect of this prioritisation on outcomes.
Methods
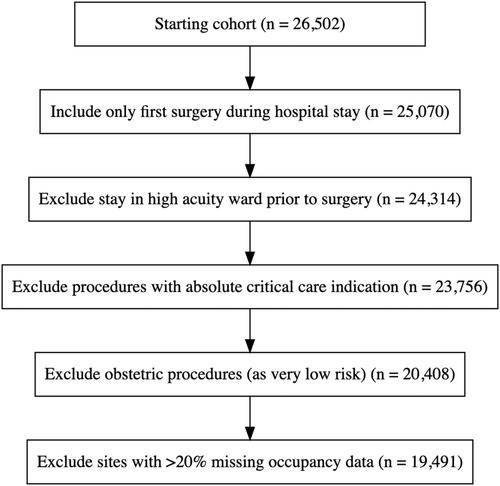
This was a prespecified analysis of an observational cohort study of adult patients undergoing inpatient surgery, conducted in 274 hospitals across the UK and Australasia during 2017. The primary outcome was postoperative morbidity at day 7. Logistic regression models were used to evaluate the relationship between critical care admission and patient and health system factors. The causal effect of critical care admission on outcome was estimated using variation in critical care occupancy as a natural experiment in an instrumental variable analysis.
Results
A total of 19,491 patients from 248 hospitals were eligible for analysis, of whom 2107 were directly admitted to critical care postoperatively. Postoperative morbidity occurred in 2829/19,491 (15%) patients. Increasing surgical risk was associated with critical care admission, as was increased availability of critical care beds (odds ratio (95%CI) 1.04 (1.01–1.06), p = 0.002) per available bed; however, the probability of admission varied significantly between hospitals (median odds ratio 3.05). There was no evidence of a difference in postoperative morbidity with critical care admission (odds ratio (95%CI) 0.91 (0.57–1.45), p = 0.710).
Discussion
Postoperative critical care admission is variable and related to bed availability. Statistical methods that adjust for unobserved confounding lowered the estimates of harm previously reported to have been associated with postoperative critical care admission. Our findings provide a rationale for a clinical trial which would evaluate any potential benefits for postoperative critical care admission for patients in whom there is no absolute indication for admission.
期刊介绍:
The official journal of the Association of Anaesthetists is Anaesthesia. It is a comprehensive international publication that covers a wide range of topics. The journal focuses on general and regional anaesthesia, as well as intensive care and pain therapy. It includes original articles that have undergone peer review, covering all aspects of these fields, including research on equipment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


