{"title":"患朝向细胞性星形细胞瘤儿童的口腔嘶哑行为","authors":"Liliana Ladner, Mebratu Daba","doi":"10.1002/cns3.20083","DOIUrl":null,"url":null,"abstract":"<p>Pilocytic astrocytomas (PA) are slow-growing gliomas that account for 15% of all central nervous system tumors.<span><sup>1</sup></span> Focal seizures are well-reported sequelae of PAs but present heterogeneously.<span><sup>2</sup></span> We describe a unique ictal “shushing” behavior in a pediatric patient with a PA of the isthmus of the cingulate gyrus.</p><p>This 14-year-old right-handed boy with no significant past medical history presented due to concern for seizures. Three to four months prior, he began experiencing daily episodes of an unusual gesture. During these episodes, he would walk toward his family or friends, place his pointer finger on his lips, and tell them to “shush” without any other vocalizations. He was aware of these episodes as they occurred but incapable of stopping them. Each episode was preceded by abdominal pain, nausea, and dizziness and followed by headaches and sleeping. Vomiting occurred after several episodes. During one episode that occurred while sleeping, his eyes rolled back for one minute, and then he awoke and promptly returned to sleep, but there were no additional seizure manifestations.</p><p>A subsequent 2-hour electroencephalogram (EEG) and continuous EEG monitoring were normal. Due to high clinical suspicion of focal seizures with impaired awareness, an MRI of the brain was ordered, and he was prescribed levetiracetam. The MRI demonstrated a lesion within the isthmus of the right cingulate gyrus that was cystic and contained a heterogeneously enhancing mural nodule (Figure 1).</p><p>Two days later, the patient underwent surgical resection of the lesion, a PA with eosinophilic granular bodies and Rosenthal fibers on histology. After the operation, he was alert but exhibited left-sided hemineglect and homonymous hemianopsia. Seven months after surgery, he stopped taking his levetiracetam, and the “shushing” behavior did not recur and there were no other seizure manifestations. Subsequent imaging demonstrated no tumor recurrence.</p><p>This patient exhibited an unusual ictal “shushing” behavior due to tumor-related epilepsy. Ictal shushing as a manifestation of a focal seizure has not been previously described in a pediatric patient. For pediatric patients with similar behaviors, both focal seizures and PAs should be on the differential.</p><p>The location of this patient's lesion in the isthmus of the right cingulate gyrus and its proximity to the temporal lobe may have contributed to his semiology. In patients with mesial temporal sclerosis, seizures arise in the hippocampus and propagate to the cortex.<span><sup>3</sup></span> Specifically, impulses from the temporal lobe may propagate through the supplementary motor area to produce index finger pointing in localization-related epilepsy.<span><sup>4</sup></span> Although similar ictal shushing has been reported as a “hush sign” in two adult patients, this report highlights the first presentation in a pediatric patient with a focal lesion.<span><sup>5</sup></span></p><p>Our patient experienced complete seizure resolution following surgery. His focal seizure type may have improved his prognosis, as a strong predictor of seizure freedom following resection of similar tumors is the presence of seizures without generalization.<span><sup>6</sup></span> Moreover, individuals with a shorter latency to operation from seizure onset have better seizure control.<span><sup>6</sup></span> This patient's favorable surgical control of his ictal shushing behavior may be related to his nongeneralized seizure type and short latency to operation. Although his seizures were not confirmed on EEG, their resolution following surgical resection suggests a plausible focal etiology.</p><p>This is the first report of a pediatric patient with ictal shushing as a manifestation of focal seizures. Future studies are warranted to characterize the appropriate type and timing of surgical intervention compared with nonsurgical antiepileptic treatment in pediatric patients with similar seizure presentations.</p><p><b>Liliana Ladner</b>: Conceptualization; data curation; investigation; methodology; validation; visualization; writing—original draft; writing—review and editing. <b>Mebratu Daba</b>: Conceptualization; data curation; funding acquisition; investigation; project administration; supervision; writing—review and editing.</p>","PeriodicalId":72232,"journal":{"name":"Annals of the Child Neurology Society","volume":"2 3","pages":"248-250"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20083","citationCount":"0","resultStr":"{\"title\":\"Ictal shushing behavior in a child with a pilocytic astrocytoma\",\"authors\":\"Liliana Ladner, Mebratu Daba\",\"doi\":\"10.1002/cns3.20083\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Pilocytic astrocytomas (PA) are slow-growing gliomas that account for 15% of all central nervous system tumors.<span><sup>1</sup></span> Focal seizures are well-reported sequelae of PAs but present heterogeneously.<span><sup>2</sup></span> We describe a unique ictal “shushing” behavior in a pediatric patient with a PA of the isthmus of the cingulate gyrus.</p><p>This 14-year-old right-handed boy with no significant past medical history presented due to concern for seizures. Three to four months prior, he began experiencing daily episodes of an unusual gesture. During these episodes, he would walk toward his family or friends, place his pointer finger on his lips, and tell them to “shush” without any other vocalizations. He was aware of these episodes as they occurred but incapable of stopping them. Each episode was preceded by abdominal pain, nausea, and dizziness and followed by headaches and sleeping. Vomiting occurred after several episodes. During one episode that occurred while sleeping, his eyes rolled back for one minute, and then he awoke and promptly returned to sleep, but there were no additional seizure manifestations.</p><p>A subsequent 2-hour electroencephalogram (EEG) and continuous EEG monitoring were normal. Due to high clinical suspicion of focal seizures with impaired awareness, an MRI of the brain was ordered, and he was prescribed levetiracetam. The MRI demonstrated a lesion within the isthmus of the right cingulate gyrus that was cystic and contained a heterogeneously enhancing mural nodule (Figure 1).</p><p>Two days later, the patient underwent surgical resection of the lesion, a PA with eosinophilic granular bodies and Rosenthal fibers on histology. After the operation, he was alert but exhibited left-sided hemineglect and homonymous hemianopsia. Seven months after surgery, he stopped taking his levetiracetam, and the “shushing” behavior did not recur and there were no other seizure manifestations. Subsequent imaging demonstrated no tumor recurrence.</p><p>This patient exhibited an unusual ictal “shushing” behavior due to tumor-related epilepsy. Ictal shushing as a manifestation of a focal seizure has not been previously described in a pediatric patient. For pediatric patients with similar behaviors, both focal seizures and PAs should be on the differential.</p><p>The location of this patient's lesion in the isthmus of the right cingulate gyrus and its proximity to the temporal lobe may have contributed to his semiology. In patients with mesial temporal sclerosis, seizures arise in the hippocampus and propagate to the cortex.<span><sup>3</sup></span> Specifically, impulses from the temporal lobe may propagate through the supplementary motor area to produce index finger pointing in localization-related epilepsy.<span><sup>4</sup></span> Although similar ictal shushing has been reported as a “hush sign” in two adult patients, this report highlights the first presentation in a pediatric patient with a focal lesion.<span><sup>5</sup></span></p><p>Our patient experienced complete seizure resolution following surgery. His focal seizure type may have improved his prognosis, as a strong predictor of seizure freedom following resection of similar tumors is the presence of seizures without generalization.<span><sup>6</sup></span> Moreover, individuals with a shorter latency to operation from seizure onset have better seizure control.<span><sup>6</sup></span> This patient's favorable surgical control of his ictal shushing behavior may be related to his nongeneralized seizure type and short latency to operation. Although his seizures were not confirmed on EEG, their resolution following surgical resection suggests a plausible focal etiology.</p><p>This is the first report of a pediatric patient with ictal shushing as a manifestation of focal seizures. Future studies are warranted to characterize the appropriate type and timing of surgical intervention compared with nonsurgical antiepileptic treatment in pediatric patients with similar seizure presentations.</p><p><b>Liliana Ladner</b>: Conceptualization; data curation; investigation; methodology; validation; visualization; writing—original draft; writing—review and editing. <b>Mebratu Daba</b>: Conceptualization; data curation; funding acquisition; investigation; project administration; supervision; writing—review and editing.</p>\",\"PeriodicalId\":72232,\"journal\":{\"name\":\"Annals of the Child Neurology Society\",\"volume\":\"2 3\",\"pages\":\"248-250\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-07-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20083\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of the Child Neurology Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20083\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Child Neurology Society","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20083","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Ictal shushing behavior in a child with a pilocytic astrocytoma
Pilocytic astrocytomas (PA) are slow-growing gliomas that account for 15% of all central nervous system tumors.1 Focal seizures are well-reported sequelae of PAs but present heterogeneously.2 We describe a unique ictal “shushing” behavior in a pediatric patient with a PA of the isthmus of the cingulate gyrus.
This 14-year-old right-handed boy with no significant past medical history presented due to concern for seizures. Three to four months prior, he began experiencing daily episodes of an unusual gesture. During these episodes, he would walk toward his family or friends, place his pointer finger on his lips, and tell them to “shush” without any other vocalizations. He was aware of these episodes as they occurred but incapable of stopping them. Each episode was preceded by abdominal pain, nausea, and dizziness and followed by headaches and sleeping. Vomiting occurred after several episodes. During one episode that occurred while sleeping, his eyes rolled back for one minute, and then he awoke and promptly returned to sleep, but there were no additional seizure manifestations.
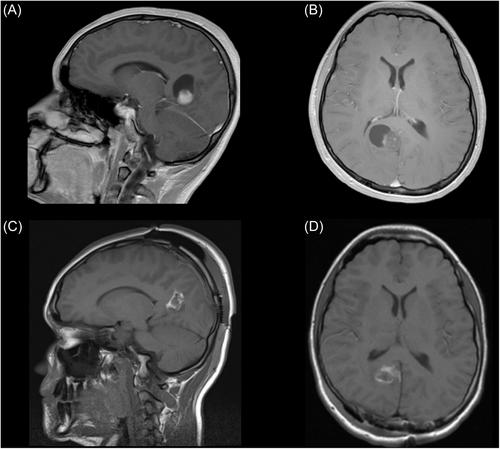
A subsequent 2-hour electroencephalogram (EEG) and continuous EEG monitoring were normal. Due to high clinical suspicion of focal seizures with impaired awareness, an MRI of the brain was ordered, and he was prescribed levetiracetam. The MRI demonstrated a lesion within the isthmus of the right cingulate gyrus that was cystic and contained a heterogeneously enhancing mural nodule (Figure 1).
Two days later, the patient underwent surgical resection of the lesion, a PA with eosinophilic granular bodies and Rosenthal fibers on histology. After the operation, he was alert but exhibited left-sided hemineglect and homonymous hemianopsia. Seven months after surgery, he stopped taking his levetiracetam, and the “shushing” behavior did not recur and there were no other seizure manifestations. Subsequent imaging demonstrated no tumor recurrence.
This patient exhibited an unusual ictal “shushing” behavior due to tumor-related epilepsy. Ictal shushing as a manifestation of a focal seizure has not been previously described in a pediatric patient. For pediatric patients with similar behaviors, both focal seizures and PAs should be on the differential.
The location of this patient's lesion in the isthmus of the right cingulate gyrus and its proximity to the temporal lobe may have contributed to his semiology. In patients with mesial temporal sclerosis, seizures arise in the hippocampus and propagate to the cortex.3 Specifically, impulses from the temporal lobe may propagate through the supplementary motor area to produce index finger pointing in localization-related epilepsy.4 Although similar ictal shushing has been reported as a “hush sign” in two adult patients, this report highlights the first presentation in a pediatric patient with a focal lesion.5
Our patient experienced complete seizure resolution following surgery. His focal seizure type may have improved his prognosis, as a strong predictor of seizure freedom following resection of similar tumors is the presence of seizures without generalization.6 Moreover, individuals with a shorter latency to operation from seizure onset have better seizure control.6 This patient's favorable surgical control of his ictal shushing behavior may be related to his nongeneralized seizure type and short latency to operation. Although his seizures were not confirmed on EEG, their resolution following surgical resection suggests a plausible focal etiology.
This is the first report of a pediatric patient with ictal shushing as a manifestation of focal seizures. Future studies are warranted to characterize the appropriate type and timing of surgical intervention compared with nonsurgical antiepileptic treatment in pediatric patients with similar seizure presentations.
Liliana Ladner: Conceptualization; data curation; investigation; methodology; validation; visualization; writing—original draft; writing—review and editing. Mebratu Daba: Conceptualization; data curation; funding acquisition; investigation; project administration; supervision; writing—review and editing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


