Vinita Bahl, Marc J Moote, Hsou Mei Hu, Darrell A Campbell
{"title":"住院病人静脉血栓栓塞风险评估中强制性与自愿性临床决策支持的影响。","authors":"Vinita Bahl, Marc J Moote, Hsou Mei Hu, Darrell A Campbell","doi":"10.1055/s-0044-1790519","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Venous thromboembolism (VTE) causes significant preventable morbidity and mortality in hospitalized patients. Assessing VTE risk is essential to initiating appropriate prophylaxis and reducing VTE outcomes. Studies show that computerized clinical decision support (CDS) can improve VTE risk assessment (RA), prophylaxis, and outcomes but few examined the effectiveness of specific design features. From 2008 to 2016, University of Michigan Health implemented CDS for VTE prevention in four stages, which alternated between voluntary and mandatory RA using the 2005 Caprini model and generated inpatient orders for risk-appropriate prophylaxis based on CHEST guidelines. This cross-sectional study evaluated the impact of mandatory versus voluntary RA on VTE prophylaxis and outcomes for adult medical and surgical patients admitted to the health system. <b>Methods</b> Interrupted time series analysis was conducted to evaluate the trend in smart order set-recommended VTE prophylaxis by CDS stage. Logistic regression with CDS stage as the primary independent variable was used in pairwise comparisons of VTE during hospitalization and within 90 days post-discharge for mandatory versus voluntary RA. Adjusted odd ratios (ORs) were calculated for total, in-hospital, and post-discharge VTE. <b>Results</b> In this study of 223,405 inpatients over 8 years, smart order set-recommended prophylaxis increased from 65 to 79%; it increased significantly when voluntary RA in Stage 1 became mandatory in Stage 2 (10.59%, <i>p</i> < 0.001) and decreased significantly when it returned to voluntary in Stage 3 (-11.24%, <i>p</i> < 0.001). The rate increased slightly when mandatory RA was reestablished in Stage 4 (0.23%, <i>p</i> = 0.935). Adjusted ORs for VTE were lower for mandatory RA versus adjacent stages with voluntary RA. The adjusted OR for Stage 2 versus Stage 1 was 14% lower ( <i>p</i> < 0.05) and versus Stage 3 was 11% lower ( <i>p</i> < 0.05). The adjusted OR for Stage 4 versus Stage 3 was 4% lower ( <i>p</i> = 0.60). These results were driven by changes in in-hospital VTE. By contrast, the incidence of post-discharge VTE increased in each successive stage. <b>Conclusion</b> Mandatory RA was more effective in improving smart order set-recommended prophylaxis and VTE outcomes, particularly in-hospital VTE. Post-discharge VTE increased despite high adherence to risk-appropriate prophylaxis, indicating that guidelines for extended, post-discharge prophylaxis are needed to further reduce VTE for hospitalized patients.</p>","PeriodicalId":94220,"journal":{"name":"TH open : companion journal to thrombosis and haemostasis","volume":"8 3","pages":"e317-e328"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392591/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Clinical Decision Support with Mandatory versus Voluntary Venous Thromboembolism Risk Assessment in Hospitalized Patients.\",\"authors\":\"Vinita Bahl, Marc J Moote, Hsou Mei Hu, Darrell A Campbell\",\"doi\":\"10.1055/s-0044-1790519\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background</b> Venous thromboembolism (VTE) causes significant preventable morbidity and mortality in hospitalized patients. Assessing VTE risk is essential to initiating appropriate prophylaxis and reducing VTE outcomes. Studies show that computerized clinical decision support (CDS) can improve VTE risk assessment (RA), prophylaxis, and outcomes but few examined the effectiveness of specific design features. From 2008 to 2016, University of Michigan Health implemented CDS for VTE prevention in four stages, which alternated between voluntary and mandatory RA using the 2005 Caprini model and generated inpatient orders for risk-appropriate prophylaxis based on CHEST guidelines. This cross-sectional study evaluated the impact of mandatory versus voluntary RA on VTE prophylaxis and outcomes for adult medical and surgical patients admitted to the health system. <b>Methods</b> Interrupted time series analysis was conducted to evaluate the trend in smart order set-recommended VTE prophylaxis by CDS stage. Logistic regression with CDS stage as the primary independent variable was used in pairwise comparisons of VTE during hospitalization and within 90 days post-discharge for mandatory versus voluntary RA. Adjusted odd ratios (ORs) were calculated for total, in-hospital, and post-discharge VTE. <b>Results</b> In this study of 223,405 inpatients over 8 years, smart order set-recommended prophylaxis increased from 65 to 79%; it increased significantly when voluntary RA in Stage 1 became mandatory in Stage 2 (10.59%, <i>p</i> < 0.001) and decreased significantly when it returned to voluntary in Stage 3 (-11.24%, <i>p</i> < 0.001). The rate increased slightly when mandatory RA was reestablished in Stage 4 (0.23%, <i>p</i> = 0.935). Adjusted ORs for VTE were lower for mandatory RA versus adjacent stages with voluntary RA. The adjusted OR for Stage 2 versus Stage 1 was 14% lower ( <i>p</i> < 0.05) and versus Stage 3 was 11% lower ( <i>p</i> < 0.05). The adjusted OR for Stage 4 versus Stage 3 was 4% lower ( <i>p</i> = 0.60). These results were driven by changes in in-hospital VTE. By contrast, the incidence of post-discharge VTE increased in each successive stage. <b>Conclusion</b> Mandatory RA was more effective in improving smart order set-recommended prophylaxis and VTE outcomes, particularly in-hospital VTE. Post-discharge VTE increased despite high adherence to risk-appropriate prophylaxis, indicating that guidelines for extended, post-discharge prophylaxis are needed to further reduce VTE for hospitalized patients.</p>\",\"PeriodicalId\":94220,\"journal\":{\"name\":\"TH open : companion journal to thrombosis and haemostasis\",\"volume\":\"8 3\",\"pages\":\"e317-e328\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-09-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392591/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"TH open : companion journal to thrombosis and haemostasis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0044-1790519\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"TH open : companion journal to thrombosis and haemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1790519","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
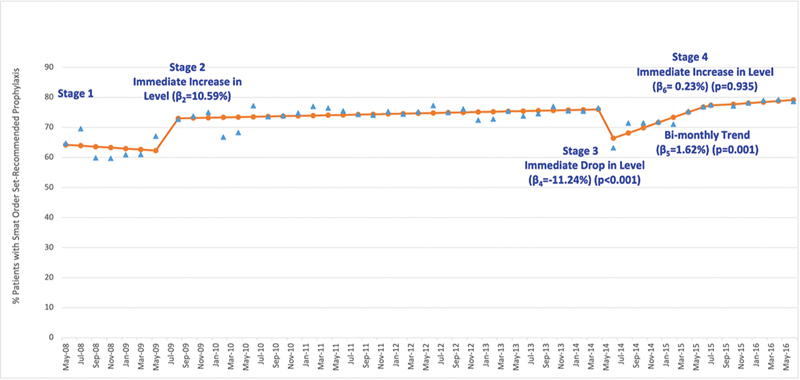
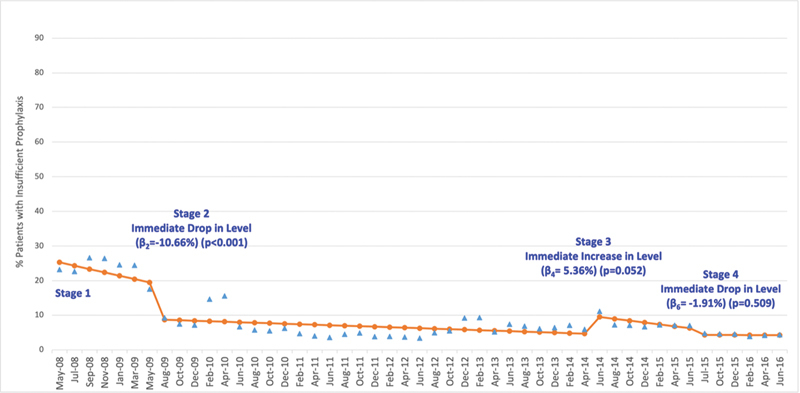
背景静脉血栓栓塞症(VTE)在住院病人中造成严重的可预防发病率和死亡率。评估 VTE 风险对于启动适当的预防措施和减少 VTE 后果至关重要。研究表明,计算机化临床决策支持(CDS)可以改善 VTE 风险评估(RA)、预防和预后,但很少有人研究具体设计功能的有效性。从 2008 年到 2016 年,密歇根大学医疗中心分四个阶段实施了用于预防 VTE 的 CDS,其中使用 2005 年的 Caprini 模型交替进行自愿和强制 RA,并根据 CHEST 指南生成风险适当的预防住院医嘱。这项横断面研究评估了强制性和自愿性 RA 对医疗系统收治的成人内科和外科病人的 VTE 预防和预后的影响。方法 采用间断时间序列分析法评估按 CDS 阶段划分的智能指令集推荐的 VTE 预防趋势。以 CDS 阶段为主要自变量的逻辑回归用于住院期间和出院后 90 天内 VTE 的配对比较,将强制 RA 与自愿 RA 进行比较。计算了总 VTE、院内 VTE 和出院后 VTE 的调整奇数比 (OR)。结果 在这项对 223,405 名住院患者进行的为期 8 年的研究中,智能医嘱组推荐的预防率从 65% 提高到 79%;当第一阶段的自愿 RA 变成第二阶段的强制 RA 时,预防率显著提高(10.59%,p p = 0.935)。与相邻阶段的自愿 RA 相比,强制性 RA 的 VTE 调整 OR 更低。第 2 阶段与第 1 阶段相比,调整后的 OR 降低了 14% ( p p p = 0.60)。这些结果是由院内 VTE 的变化引起的。相比之下,出院后 VTE 的发生率在每个连续阶段都有所增加。结论 强制性 RA 更有效地改善了智能订单组推荐的预防措施和 VTE 结果,尤其是院内 VTE。尽管对风险适当的预防措施的依从性很高,但出院后 VTE 的发生率仍有所增加,这表明需要制定出院后延长预防措施的指南,以进一步减少住院患者的 VTE。
Impact of Clinical Decision Support with Mandatory versus Voluntary Venous Thromboembolism Risk Assessment in Hospitalized Patients.
Background Venous thromboembolism (VTE) causes significant preventable morbidity and mortality in hospitalized patients. Assessing VTE risk is essential to initiating appropriate prophylaxis and reducing VTE outcomes. Studies show that computerized clinical decision support (CDS) can improve VTE risk assessment (RA), prophylaxis, and outcomes but few examined the effectiveness of specific design features. From 2008 to 2016, University of Michigan Health implemented CDS for VTE prevention in four stages, which alternated between voluntary and mandatory RA using the 2005 Caprini model and generated inpatient orders for risk-appropriate prophylaxis based on CHEST guidelines. This cross-sectional study evaluated the impact of mandatory versus voluntary RA on VTE prophylaxis and outcomes for adult medical and surgical patients admitted to the health system. Methods Interrupted time series analysis was conducted to evaluate the trend in smart order set-recommended VTE prophylaxis by CDS stage. Logistic regression with CDS stage as the primary independent variable was used in pairwise comparisons of VTE during hospitalization and within 90 days post-discharge for mandatory versus voluntary RA. Adjusted odd ratios (ORs) were calculated for total, in-hospital, and post-discharge VTE. Results In this study of 223,405 inpatients over 8 years, smart order set-recommended prophylaxis increased from 65 to 79%; it increased significantly when voluntary RA in Stage 1 became mandatory in Stage 2 (10.59%, p < 0.001) and decreased significantly when it returned to voluntary in Stage 3 (-11.24%, p < 0.001). The rate increased slightly when mandatory RA was reestablished in Stage 4 (0.23%, p = 0.935). Adjusted ORs for VTE were lower for mandatory RA versus adjacent stages with voluntary RA. The adjusted OR for Stage 2 versus Stage 1 was 14% lower ( p < 0.05) and versus Stage 3 was 11% lower ( p < 0.05). The adjusted OR for Stage 4 versus Stage 3 was 4% lower ( p = 0.60). These results were driven by changes in in-hospital VTE. By contrast, the incidence of post-discharge VTE increased in each successive stage. Conclusion Mandatory RA was more effective in improving smart order set-recommended prophylaxis and VTE outcomes, particularly in-hospital VTE. Post-discharge VTE increased despite high adherence to risk-appropriate prophylaxis, indicating that guidelines for extended, post-discharge prophylaxis are needed to further reduce VTE for hospitalized patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


