{"title":"为预防同种异体造血细胞移植中的骨质流失,移植前使用唑来膦酸盐与观察法的随机对照试验。","authors":"Niranjan Khaire, Urmimala Bhattacharjee, Arjun Dinesan, Anindita Sinha, Sanjay Bhadada, Andrew Pardeep, Prashant Chhabra, Ritika Sharma, Renaissa De, Shaweta Kaundal, Kripa Shanker Kasudhan, Lekshmon Ks, Charanpreet Singh, Aditya Jandial, Arihant Jain, Gaurav Prakash, Alka Khadwal, Amol Patil, Pankaj Malhotra, Deepesh Lad","doi":"10.31547/bct-2024-003","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Approximately half of allogeneic hematopoietic cell transplantation (HCT) recipients experience significant bone loss in the early post-HCT period. Only recently have international guidelines started recommending early screening. However, the guidance for intervention remains conservative. In this study, we sought to evaluate the efficacy of pre-transplant prophylactic zoledronate in preventing early bone loss in allogeneic HCT recipients.</p><p><strong>Methods: </strong>This was an open-label, investigator-initiated, phase 2 randomized controlled trial (RCT) of prophylactic zoledronate versus observation to prevent bone loss in allogeneic HCT recipients. Recipients aged ≥ 18 years of age were included after informed consent and randomized to prophylactic zoledronate 4 mg pre-HCT or observation in a 1:1 ratio. The primary outcome of the study was bone mineral density (BMD) loss at the femoral neck (FN), total hip (TH), and lumbar spine (LS), as assessed using dual-energy X-ray absorptiometry (DXA) on day+100 post-HCT. The secondary outcomes included BMD loss on day+365 and Z scores on day+100 and day+365 at the FN, TH, and LS sites.</p><p><strong>Results: </strong>The trial was terminated because the interim analysis showed a significant benefit in the intervention arm, with 50% planned recruitment. A total of 40 patients were randomized to the zoledronate and control arms. Both arms were matched for age, sex, diagnosis, pre-HCT steroid exposure, body mass index, human leukocyte antigen (HLA) match, and conditioning intensity. The grade 2-4 acute graft versus host disease (GVHD) incidences were comparable. The primary endpoint of BMD loss at FN and TH at day+100 was significant (5.62% vs. -6.78%, <i>p</i> = 0.009, -1.59 vs. -3.98, <i>p</i> = 0.016, respectively). There was no difference in the secondary endpoint of BMD loss on day+365 compared to that on day+100 or baseline at any BMD site. There was no difference in the Z-scores at any site on day+100 or day+365.</p><p><strong>Conclusions: </strong>Prophylactic zoledronate prevented early bone loss on day+100. The indicated preemptive zoledronate beyond day+100 in recipients prevented further bone loss. Patients receiving prophylactic zoledronate may benefit from a supplementary dose of the indicated preemptive zoledronate.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"7 3","pages":"87-94"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11384127/pdf/","citationCount":"0","resultStr":"{\"title\":\"Randomized controlled trial of pre-transplant zoledronate versus observation for prevention of bone loss in allogeneic hematopoietic cell transplantation.\",\"authors\":\"Niranjan Khaire, Urmimala Bhattacharjee, Arjun Dinesan, Anindita Sinha, Sanjay Bhadada, Andrew Pardeep, Prashant Chhabra, Ritika Sharma, Renaissa De, Shaweta Kaundal, Kripa Shanker Kasudhan, Lekshmon Ks, Charanpreet Singh, Aditya Jandial, Arihant Jain, Gaurav Prakash, Alka Khadwal, Amol Patil, Pankaj Malhotra, Deepesh Lad\",\"doi\":\"10.31547/bct-2024-003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Approximately half of allogeneic hematopoietic cell transplantation (HCT) recipients experience significant bone loss in the early post-HCT period. Only recently have international guidelines started recommending early screening. However, the guidance for intervention remains conservative. In this study, we sought to evaluate the efficacy of pre-transplant prophylactic zoledronate in preventing early bone loss in allogeneic HCT recipients.</p><p><strong>Methods: </strong>This was an open-label, investigator-initiated, phase 2 randomized controlled trial (RCT) of prophylactic zoledronate versus observation to prevent bone loss in allogeneic HCT recipients. Recipients aged ≥ 18 years of age were included after informed consent and randomized to prophylactic zoledronate 4 mg pre-HCT or observation in a 1:1 ratio. The primary outcome of the study was bone mineral density (BMD) loss at the femoral neck (FN), total hip (TH), and lumbar spine (LS), as assessed using dual-energy X-ray absorptiometry (DXA) on day+100 post-HCT. The secondary outcomes included BMD loss on day+365 and Z scores on day+100 and day+365 at the FN, TH, and LS sites.</p><p><strong>Results: </strong>The trial was terminated because the interim analysis showed a significant benefit in the intervention arm, with 50% planned recruitment. A total of 40 patients were randomized to the zoledronate and control arms. Both arms were matched for age, sex, diagnosis, pre-HCT steroid exposure, body mass index, human leukocyte antigen (HLA) match, and conditioning intensity. The grade 2-4 acute graft versus host disease (GVHD) incidences were comparable. The primary endpoint of BMD loss at FN and TH at day+100 was significant (5.62% vs. -6.78%, <i>p</i> = 0.009, -1.59 vs. -3.98, <i>p</i> = 0.016, respectively). There was no difference in the secondary endpoint of BMD loss on day+365 compared to that on day+100 or baseline at any BMD site. There was no difference in the Z-scores at any site on day+100 or day+365.</p><p><strong>Conclusions: </strong>Prophylactic zoledronate prevented early bone loss on day+100. The indicated preemptive zoledronate beyond day+100 in recipients prevented further bone loss. Patients receiving prophylactic zoledronate may benefit from a supplementary dose of the indicated preemptive zoledronate.</p>\",\"PeriodicalId\":72423,\"journal\":{\"name\":\"Blood cell therapy\",\"volume\":\"7 3\",\"pages\":\"87-94\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-07-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11384127/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31547/bct-2024-003\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/25 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2024-003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/25 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:大约一半的异基因造血细胞移植(HCT)受者在移植后早期会出现明显的骨质流失。直到最近,国际指南才开始建议进行早期筛查。然而,有关干预措施的指导仍很保守。在这项研究中,我们试图评估移植前预防性使用唑来膦酸钠预防同种异体 HCT 受者早期骨质流失的疗效:这是一项由研究者发起的开放标签 2 期随机对照试验(RCT),研究对象为预防性使用唑来膦酸钠与观察治疗相比,预防异基因 HCT 受者骨质流失的效果。年龄≥18岁的受者在知情同意后被纳入试验,并按1:1的比例随机接受接受造血干细胞移植前预防性唑来膦酸钠4毫克或观察治疗。研究的主要结果是股骨颈(FN)、全髋(TH)和腰椎(LS)的骨矿物质密度(BMD)损失,采用双能 X 射线吸收测定法(DXA)在造血干细胞移植后第 100 天进行评估。次要结果包括第+365天的BMD损失以及第+100天和第+365天FN、TH和LS部位的Z评分:由于中期分析显示干预组有显著疗效,试验终止,计划招募人数为 50%。共有 40 名患者被随机分配到唑来膦酸钠治疗组和对照组。两组患者的年龄、性别、诊断、HCT前类固醇暴露、体重指数、人类白细胞抗原(HLA)匹配度和调理强度均相匹配。2-4级急性移植物抗宿主疾病(GVHD)发生率相当。主要终点FN和TH在100天+时的BMD损失显著(分别为5.62% vs. -6.78%,p = 0.009;-1.59 vs. -3.98,p = 0.016)。与第+100天或任何BMD部位的基线相比,第+365天的BMD损失这一次要终点均无差异。第+100天或第+365天任何部位的Z-scores均无差异:结论:预防性唑来膦酸钠可预防第+100天的早期骨质流失。结论:预防性使用唑来膦酸钠可防止第 100 天的早期骨质流失,而在第 100 天之后,受者使用指定的唑来膦酸钠可防止骨质进一步流失。接受预防性唑来膦酸盐治疗的患者可能会从补充服用指定剂量的唑来膦酸盐中获益。
Randomized controlled trial of pre-transplant zoledronate versus observation for prevention of bone loss in allogeneic hematopoietic cell transplantation.
Background: Approximately half of allogeneic hematopoietic cell transplantation (HCT) recipients experience significant bone loss in the early post-HCT period. Only recently have international guidelines started recommending early screening. However, the guidance for intervention remains conservative. In this study, we sought to evaluate the efficacy of pre-transplant prophylactic zoledronate in preventing early bone loss in allogeneic HCT recipients.
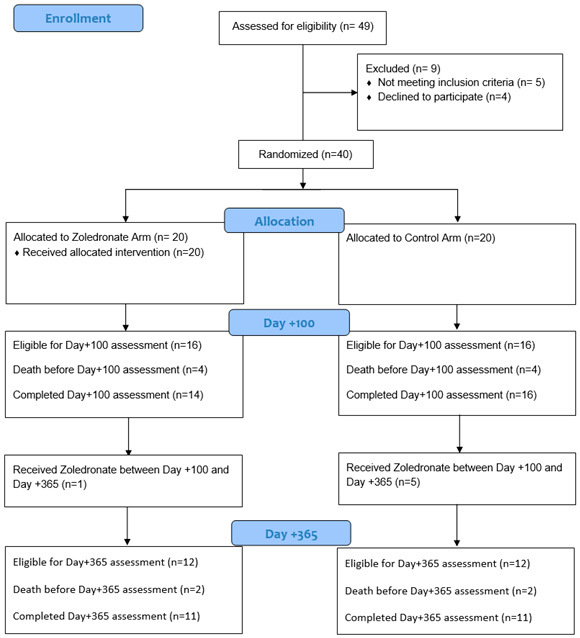
Methods: This was an open-label, investigator-initiated, phase 2 randomized controlled trial (RCT) of prophylactic zoledronate versus observation to prevent bone loss in allogeneic HCT recipients. Recipients aged ≥ 18 years of age were included after informed consent and randomized to prophylactic zoledronate 4 mg pre-HCT or observation in a 1:1 ratio. The primary outcome of the study was bone mineral density (BMD) loss at the femoral neck (FN), total hip (TH), and lumbar spine (LS), as assessed using dual-energy X-ray absorptiometry (DXA) on day+100 post-HCT. The secondary outcomes included BMD loss on day+365 and Z scores on day+100 and day+365 at the FN, TH, and LS sites.
Results: The trial was terminated because the interim analysis showed a significant benefit in the intervention arm, with 50% planned recruitment. A total of 40 patients were randomized to the zoledronate and control arms. Both arms were matched for age, sex, diagnosis, pre-HCT steroid exposure, body mass index, human leukocyte antigen (HLA) match, and conditioning intensity. The grade 2-4 acute graft versus host disease (GVHD) incidences were comparable. The primary endpoint of BMD loss at FN and TH at day+100 was significant (5.62% vs. -6.78%, p = 0.009, -1.59 vs. -3.98, p = 0.016, respectively). There was no difference in the secondary endpoint of BMD loss on day+365 compared to that on day+100 or baseline at any BMD site. There was no difference in the Z-scores at any site on day+100 or day+365.
Conclusions: Prophylactic zoledronate prevented early bone loss on day+100. The indicated preemptive zoledronate beyond day+100 in recipients prevented further bone loss. Patients receiving prophylactic zoledronate may benefit from a supplementary dose of the indicated preemptive zoledronate.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


