Quincy A Hathaway, Ankush D Jamthikar, Nivedita Rajiv, Bernard R Chaitman, Jeffrey L Carson, Naveena Yanamala, Partho P Sengupta
{"title":"心脏超声组学用于急性心肌梗死风险分层和全因死亡率预测:一项可行性研究。","authors":"Quincy A Hathaway, Ankush D Jamthikar, Nivedita Rajiv, Bernard R Chaitman, Jeffrey L Carson, Naveena Yanamala, Partho P Sengupta","doi":"10.1186/s44156-024-00057-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current risk stratification tools for acute myocardial infarction (AMI) have limitations, particularly in predicting mortality. This study utilizes cardiac ultrasound radiomics (i.e., ultrasomics) to risk stratify AMI patients when predicting all-cause mortality.</p><p><strong>Results: </strong>The study included 197 patients: (a) retrospective internal cohort (n = 155) of non-ST-elevation myocardial infarction (n = 63) and ST-elevation myocardial infarction (n = 92) patients, and (b) external cohort from the multicenter Door-To-Unload in ST-segment-elevation myocardial infarction [DTU-STEMI] Pilot Trial (n = 42). Echocardiography images of apical 2, 3, and 4-chamber were processed through an automated deep-learning pipeline to extract ultrasomic features. Unsupervised machine learning (topological data analysis) generated AMI clusters followed by a supervised classifier to generate individual predicted probabilities. Validation included assessing the incremental value of predicted probabilities over the Global Registry of Acute Coronary Events (GRACE) risk score 2.0 to predict 1-year all-cause mortality in the internal cohort and infarct size in the external cohort. Three phenogroups were identified: Cluster A (high-risk), Cluster B (intermediate-risk), and Cluster C (low-risk). Cluster A patients had decreased LV ejection fraction (P < 0.01) and global longitudinal strain (P = 0.03) and increased mortality at 1-year (log rank P = 0.05). Ultrasomics features alone (C-Index: 0.74 vs. 0.70, P = 0.04) and combined with global longitudinal strain (C-Index: 0.81 vs. 0.70, P < 0.01) increased prediction of mortality beyond the GRACE 2.0 score. In the DTU-STEMI clinical trial, Cluster A was associated with larger infarct size (> 10% LV mass, P < 0.01), compared to remaining clusters.</p><p><strong>Conclusions: </strong>Ultrasomics-based phenogroup clustering, augmented by TDA and supervised machine learning, provides a novel approach for AMI risk stratification.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"11 1","pages":"22"},"PeriodicalIF":2.4000,"publicationDate":"2024-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11403884/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cardiac ultrasomics for acute myocardial infarction risk stratification and prediction of all-cause mortality: a feasibility study.\",\"authors\":\"Quincy A Hathaway, Ankush D Jamthikar, Nivedita Rajiv, Bernard R Chaitman, Jeffrey L Carson, Naveena Yanamala, Partho P Sengupta\",\"doi\":\"10.1186/s44156-024-00057-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Current risk stratification tools for acute myocardial infarction (AMI) have limitations, particularly in predicting mortality. This study utilizes cardiac ultrasound radiomics (i.e., ultrasomics) to risk stratify AMI patients when predicting all-cause mortality.</p><p><strong>Results: </strong>The study included 197 patients: (a) retrospective internal cohort (n = 155) of non-ST-elevation myocardial infarction (n = 63) and ST-elevation myocardial infarction (n = 92) patients, and (b) external cohort from the multicenter Door-To-Unload in ST-segment-elevation myocardial infarction [DTU-STEMI] Pilot Trial (n = 42). Echocardiography images of apical 2, 3, and 4-chamber were processed through an automated deep-learning pipeline to extract ultrasomic features. Unsupervised machine learning (topological data analysis) generated AMI clusters followed by a supervised classifier to generate individual predicted probabilities. Validation included assessing the incremental value of predicted probabilities over the Global Registry of Acute Coronary Events (GRACE) risk score 2.0 to predict 1-year all-cause mortality in the internal cohort and infarct size in the external cohort. Three phenogroups were identified: Cluster A (high-risk), Cluster B (intermediate-risk), and Cluster C (low-risk). Cluster A patients had decreased LV ejection fraction (P < 0.01) and global longitudinal strain (P = 0.03) and increased mortality at 1-year (log rank P = 0.05). Ultrasomics features alone (C-Index: 0.74 vs. 0.70, P = 0.04) and combined with global longitudinal strain (C-Index: 0.81 vs. 0.70, P < 0.01) increased prediction of mortality beyond the GRACE 2.0 score. In the DTU-STEMI clinical trial, Cluster A was associated with larger infarct size (> 10% LV mass, P < 0.01), compared to remaining clusters.</p><p><strong>Conclusions: </strong>Ultrasomics-based phenogroup clustering, augmented by TDA and supervised machine learning, provides a novel approach for AMI risk stratification.</p>\",\"PeriodicalId\":45749,\"journal\":{\"name\":\"Echo Research and Practice\",\"volume\":\"11 1\",\"pages\":\"22\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-09-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11403884/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Echo Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44156-024-00057-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-024-00057-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:目前的急性心肌梗死(AMI)风险分层工具存在局限性,尤其是在预测死亡率方面。本研究利用心脏超声放射组学(即超声组学)对急性心肌梗死患者进行风险分层,预测全因死亡率:研究纳入了 197 名患者:(a)非 ST 段抬高型心肌梗死(63 例)和 ST 段抬高型心肌梗死(92 例)患者的回顾性内部队列(n = 155);(b)多中心 ST 段抬高型心肌梗死[DTU-STEMI] 先导试验(Door-To-Unload in ST-segment-elevation myocardial infarction [DTU-STEMI] Pilot Trial)的外部队列(n = 42)。心尖二腔、三腔和四腔超声心动图图像通过自动深度学习管道进行处理,以提取超声心动图特征。无监督机器学习(拓扑数据分析)生成急性心肌梗死集群,然后由监督分类器生成单个预测概率。验证包括评估预测概率相对于全球急性冠脉事件登记(GRACE)风险评分 2.0 的增量值,以预测内部队列中的 1 年全因死亡率和外部队列中的梗死面积。确定了三个表型组:A组(高危)、B组(中危)和C组(低危)。A组患者的左心室射血分数下降(P 10%),左心室质量下降(P基于超体组学的表型组聚类法,辅以 TDA 和有监督的机器学习,为 AMI 风险分层提供了一种新方法。
Cardiac ultrasomics for acute myocardial infarction risk stratification and prediction of all-cause mortality: a feasibility study.
Background: Current risk stratification tools for acute myocardial infarction (AMI) have limitations, particularly in predicting mortality. This study utilizes cardiac ultrasound radiomics (i.e., ultrasomics) to risk stratify AMI patients when predicting all-cause mortality.
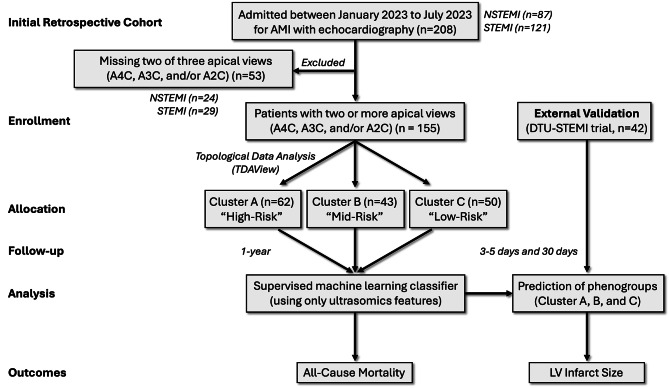
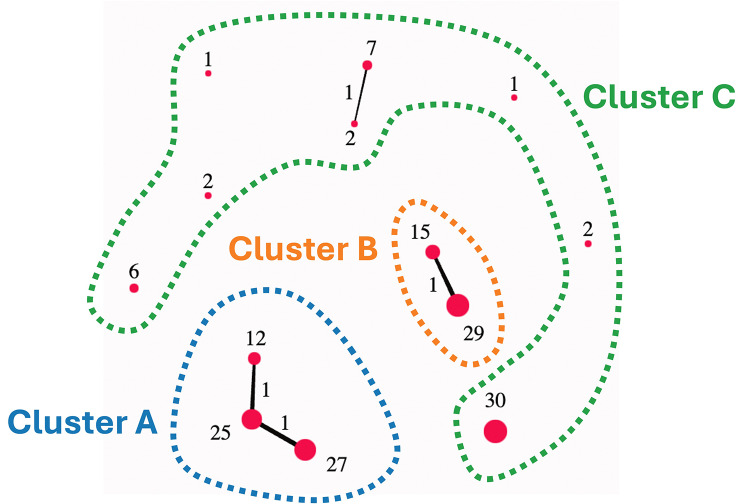
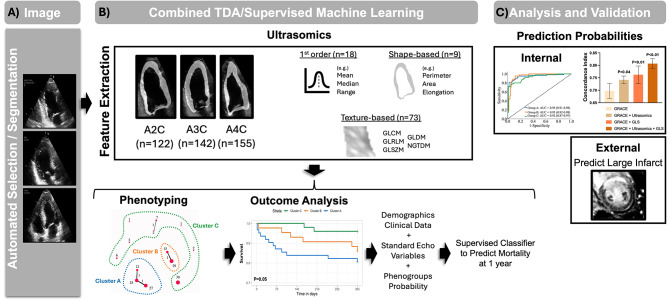
Results: The study included 197 patients: (a) retrospective internal cohort (n = 155) of non-ST-elevation myocardial infarction (n = 63) and ST-elevation myocardial infarction (n = 92) patients, and (b) external cohort from the multicenter Door-To-Unload in ST-segment-elevation myocardial infarction [DTU-STEMI] Pilot Trial (n = 42). Echocardiography images of apical 2, 3, and 4-chamber were processed through an automated deep-learning pipeline to extract ultrasomic features. Unsupervised machine learning (topological data analysis) generated AMI clusters followed by a supervised classifier to generate individual predicted probabilities. Validation included assessing the incremental value of predicted probabilities over the Global Registry of Acute Coronary Events (GRACE) risk score 2.0 to predict 1-year all-cause mortality in the internal cohort and infarct size in the external cohort. Three phenogroups were identified: Cluster A (high-risk), Cluster B (intermediate-risk), and Cluster C (low-risk). Cluster A patients had decreased LV ejection fraction (P < 0.01) and global longitudinal strain (P = 0.03) and increased mortality at 1-year (log rank P = 0.05). Ultrasomics features alone (C-Index: 0.74 vs. 0.70, P = 0.04) and combined with global longitudinal strain (C-Index: 0.81 vs. 0.70, P < 0.01) increased prediction of mortality beyond the GRACE 2.0 score. In the DTU-STEMI clinical trial, Cluster A was associated with larger infarct size (> 10% LV mass, P < 0.01), compared to remaining clusters.
Conclusions: Ultrasomics-based phenogroup clustering, augmented by TDA and supervised machine learning, provides a novel approach for AMI risk stratification.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


