{"title":"在 2 型糖尿病心力衰竭患者的标准治疗中添加 SGLT-2 抑制剂的成本效用和预算影响分析:利用泰国国家数据库的洞察力。","authors":"Tanawan Kongmalai, Juthamas Prawjaeng, Phorntida Hadnorntun, Pattara Leelahavarong, Usa Chaikledkaew, Ammarin Thakkinstian, Varalak Srinonprasert","doi":"10.1007/s41669-024-00526-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Heart failure (HF) in type 2 diabetes (T2D) patients poses a significant clinical and financial burden. While sodium-glucose cotransporter-2 inhibitors (SGLT2i) have shown cardiovascular benefits in trials, they are not included in Thailand's National List of Essential Medicines (NLEM), and their value-for-money remains unassessed.</p><p><strong>Objective: </strong>This study aims to evaluate the cost-utility of adding SGLT2i to the standard treatment for T2D-HF patients in Thailand.</p><p><strong>Methods: </strong>A Markov model with 3-month cycles and a lifetime horizon was conducted from a societal perspective. Efficacy data came from a systematic review and meta-analysis. Transition probabilities and direct medical costs were derived from the National Health Security Office database, while direct non-medical costs and utility were collected through patient interviews at Siriraj hospital to reflect Thailand's context. The main outcomes were incremental costs, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER). A sensitivity and budget impact analysis were also performed.</p><p><strong>Results: </strong>Canagliflozin led to the highest increase in QALYs, at 1.21 years, followed by dapagliflozin (0.54 years) and empagliflozin (0.06 years). Collectively, SGLT2i yielded an increase of 0.41 QALYs. Canagliflozin incurred the highest additional treatment cost at United States dollars (US$)5600, followed by dapagliflozin (US$3547) and empagliflozin (US$2694). The ICERs for canagliflozin, dapagliflozin, empagliflozin, and overall SGLT2i were US$4632, US$6430, US$48,952, and US$8480 per QALY gained, respectively. SGLT2i were not cost-effective compared with Thailand's willingness-to-pay threshold of US$4564 per QALY gained. However, threshold analysis indicates that the costs of canagliflozin, dapagliflozin, empagliflozin, and overall SGLT-2i should be reduced by 2.3%, 38.2%, 90.2%, and 55.6%, respectively, to be cost-effective. Budget impact analysis revealed that the total budget for treating T2D patients with HF over 5 years is US$15.6 million.</p><p><strong>Conclusions: </strong>Adding SGLT2i to standard treatment reduced HF hospitalization and mortality rates and improved QALYs in T2D-HF patients. Nevertheless, they would not be cost-effective at current prices in Thailand.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"69-81"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717763/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-Utility and Budget Impact Analysis of Adding SGLT-2 Inhibitors to Standard Treatment in Type 2 Diabetes Patients with Heart Failure: Utilizing National Database Insights from Thailand.\",\"authors\":\"Tanawan Kongmalai, Juthamas Prawjaeng, Phorntida Hadnorntun, Pattara Leelahavarong, Usa Chaikledkaew, Ammarin Thakkinstian, Varalak Srinonprasert\",\"doi\":\"10.1007/s41669-024-00526-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Heart failure (HF) in type 2 diabetes (T2D) patients poses a significant clinical and financial burden. While sodium-glucose cotransporter-2 inhibitors (SGLT2i) have shown cardiovascular benefits in trials, they are not included in Thailand's National List of Essential Medicines (NLEM), and their value-for-money remains unassessed.</p><p><strong>Objective: </strong>This study aims to evaluate the cost-utility of adding SGLT2i to the standard treatment for T2D-HF patients in Thailand.</p><p><strong>Methods: </strong>A Markov model with 3-month cycles and a lifetime horizon was conducted from a societal perspective. Efficacy data came from a systematic review and meta-analysis. Transition probabilities and direct medical costs were derived from the National Health Security Office database, while direct non-medical costs and utility were collected through patient interviews at Siriraj hospital to reflect Thailand's context. The main outcomes were incremental costs, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER). A sensitivity and budget impact analysis were also performed.</p><p><strong>Results: </strong>Canagliflozin led to the highest increase in QALYs, at 1.21 years, followed by dapagliflozin (0.54 years) and empagliflozin (0.06 years). Collectively, SGLT2i yielded an increase of 0.41 QALYs. Canagliflozin incurred the highest additional treatment cost at United States dollars (US$)5600, followed by dapagliflozin (US$3547) and empagliflozin (US$2694). The ICERs for canagliflozin, dapagliflozin, empagliflozin, and overall SGLT2i were US$4632, US$6430, US$48,952, and US$8480 per QALY gained, respectively. SGLT2i were not cost-effective compared with Thailand's willingness-to-pay threshold of US$4564 per QALY gained. However, threshold analysis indicates that the costs of canagliflozin, dapagliflozin, empagliflozin, and overall SGLT-2i should be reduced by 2.3%, 38.2%, 90.2%, and 55.6%, respectively, to be cost-effective. Budget impact analysis revealed that the total budget for treating T2D patients with HF over 5 years is US$15.6 million.</p><p><strong>Conclusions: </strong>Adding SGLT2i to standard treatment reduced HF hospitalization and mortality rates and improved QALYs in T2D-HF patients. Nevertheless, they would not be cost-effective at current prices in Thailand.</p>\",\"PeriodicalId\":19770,\"journal\":{\"name\":\"PharmacoEconomics Open\",\"volume\":\" \",\"pages\":\"69-81\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717763/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s41669-024-00526-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-024-00526-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
Cost-Utility and Budget Impact Analysis of Adding SGLT-2 Inhibitors to Standard Treatment in Type 2 Diabetes Patients with Heart Failure: Utilizing National Database Insights from Thailand.
Background: Heart failure (HF) in type 2 diabetes (T2D) patients poses a significant clinical and financial burden. While sodium-glucose cotransporter-2 inhibitors (SGLT2i) have shown cardiovascular benefits in trials, they are not included in Thailand's National List of Essential Medicines (NLEM), and their value-for-money remains unassessed.
Objective: This study aims to evaluate the cost-utility of adding SGLT2i to the standard treatment for T2D-HF patients in Thailand.
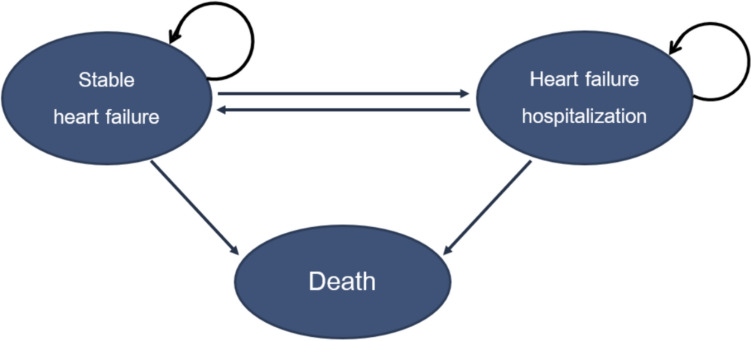
Methods: A Markov model with 3-month cycles and a lifetime horizon was conducted from a societal perspective. Efficacy data came from a systematic review and meta-analysis. Transition probabilities and direct medical costs were derived from the National Health Security Office database, while direct non-medical costs and utility were collected through patient interviews at Siriraj hospital to reflect Thailand's context. The main outcomes were incremental costs, quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratio (ICER). A sensitivity and budget impact analysis were also performed.
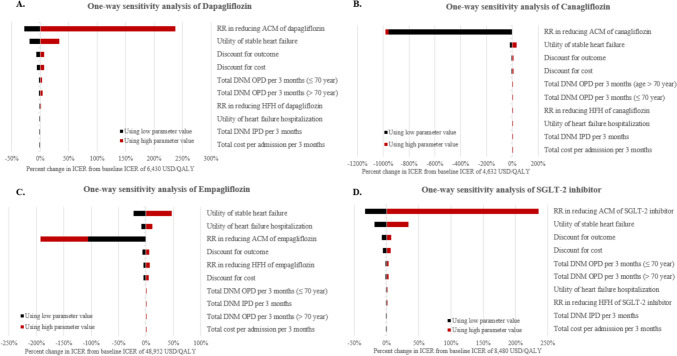
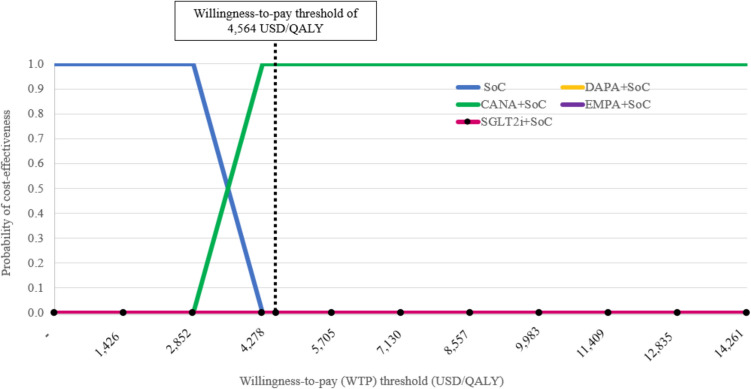
Results: Canagliflozin led to the highest increase in QALYs, at 1.21 years, followed by dapagliflozin (0.54 years) and empagliflozin (0.06 years). Collectively, SGLT2i yielded an increase of 0.41 QALYs. Canagliflozin incurred the highest additional treatment cost at United States dollars (US$)5600, followed by dapagliflozin (US$3547) and empagliflozin (US$2694). The ICERs for canagliflozin, dapagliflozin, empagliflozin, and overall SGLT2i were US$4632, US$6430, US$48,952, and US$8480 per QALY gained, respectively. SGLT2i were not cost-effective compared with Thailand's willingness-to-pay threshold of US$4564 per QALY gained. However, threshold analysis indicates that the costs of canagliflozin, dapagliflozin, empagliflozin, and overall SGLT-2i should be reduced by 2.3%, 38.2%, 90.2%, and 55.6%, respectively, to be cost-effective. Budget impact analysis revealed that the total budget for treating T2D patients with HF over 5 years is US$15.6 million.
Conclusions: Adding SGLT2i to standard treatment reduced HF hospitalization and mortality rates and improved QALYs in T2D-HF patients. Nevertheless, they would not be cost-effective at current prices in Thailand.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


