Luke J. Vlismas, Michael Potter, Mark R. Loewenthal, Katie Wilson, Kelleigh Allport, Donna Gillies, Dane Cook, Stephen Philcox, Steven Bollipo, Nicholas J. Talley
{"title":"在一家三级医院接受内镜监测的低度发育不良巴雷特食道患者的预后:一项回顾性队列研究。","authors":"Luke J. Vlismas, Michael Potter, Mark R. Loewenthal, Katie Wilson, Kelleigh Allport, Donna Gillies, Dane Cook, Stephen Philcox, Steven Bollipo, Nicholas J. Talley","doi":"10.1111/imj.16532","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background and Aim</h3>\n \n <p>Barrett's oesophagus predisposes individuals to oesophageal adenocarcinoma (OAC), with the risk of progression to malignancy increasing with the degree of dysplasia, categorized as either low-grade dysplasia (LGD) or high-grade dysplasia (HGD). The reported incidence of progression to OAC in LGD ranges from 0.02% to 11.43% per annum. In patients with LGD, Australian guidelines recommend 6-monthly endoscopic surveillance. We aimed to describe the surveillance practices within a tertiary centre, and to determine the predictive value of surveillance as well as other risk factors for progression.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Endoscopy and pathology databases were searched over a 10-year period to collate all cases of Barrett's oesophagus with LGD. Medical records were reviewed to document patient factors and endoscopic and histologic details. Because follow-up times varied greatly, survival analysis techniques were employed.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Fifty-nine patients were found to have LGD. Thirteen patients (22.0%) progressed to either HGD or OAC (10 (16.9%) and three (5.1%) respectively); the annual incidence rates of progression to HGD/OAC and OAC were 5.5% and 1.1% respectively. All patients who developed OAC had non-guideline-adherent surveillance. A Cox model found only two predictors of progression: (i) guideline-adherent surveillance, performed in 16 (27.1%), detected progression to HGD/OAC four times earlier than non-guideline-adherent surveillance (95% confidence interval (CI) = 1.3–12.3; <i>P</i> = 0.016). (ii) The detection of visible lesions at exit endoscopy independently predicted progression (hazard ratio = 6.5; 95% CI = 1.9–22.8; <i>P</i> = 0.003).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Barrett's oesophagus with LGD poses a significant risk of progression to HGD/OAC. Guideline-recommended surveillance is effective, but is difficult to adhere to. Clinical predictors for those who are more likely to progress are yet to be defined.</p>\n </section>\n </div>","PeriodicalId":13625,"journal":{"name":"Internal Medicine Journal","volume":"54 11","pages":"1867-1875"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/imj.16532","citationCount":"0","resultStr":"{\"title\":\"Outcomes of patients with Barrett's oesophagus with low-grade dysplasia undergoing endoscopic surveillance in a tertiary centre: a retrospective cohort study\",\"authors\":\"Luke J. Vlismas, Michael Potter, Mark R. Loewenthal, Katie Wilson, Kelleigh Allport, Donna Gillies, Dane Cook, Stephen Philcox, Steven Bollipo, Nicholas J. Talley\",\"doi\":\"10.1111/imj.16532\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background and Aim</h3>\\n \\n <p>Barrett's oesophagus predisposes individuals to oesophageal adenocarcinoma (OAC), with the risk of progression to malignancy increasing with the degree of dysplasia, categorized as either low-grade dysplasia (LGD) or high-grade dysplasia (HGD). The reported incidence of progression to OAC in LGD ranges from 0.02% to 11.43% per annum. In patients with LGD, Australian guidelines recommend 6-monthly endoscopic surveillance. We aimed to describe the surveillance practices within a tertiary centre, and to determine the predictive value of surveillance as well as other risk factors for progression.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Endoscopy and pathology databases were searched over a 10-year period to collate all cases of Barrett's oesophagus with LGD. Medical records were reviewed to document patient factors and endoscopic and histologic details. Because follow-up times varied greatly, survival analysis techniques were employed.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Fifty-nine patients were found to have LGD. Thirteen patients (22.0%) progressed to either HGD or OAC (10 (16.9%) and three (5.1%) respectively); the annual incidence rates of progression to HGD/OAC and OAC were 5.5% and 1.1% respectively. All patients who developed OAC had non-guideline-adherent surveillance. A Cox model found only two predictors of progression: (i) guideline-adherent surveillance, performed in 16 (27.1%), detected progression to HGD/OAC four times earlier than non-guideline-adherent surveillance (95% confidence interval (CI) = 1.3–12.3; <i>P</i> = 0.016). (ii) The detection of visible lesions at exit endoscopy independently predicted progression (hazard ratio = 6.5; 95% CI = 1.9–22.8; <i>P</i> = 0.003).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Barrett's oesophagus with LGD poses a significant risk of progression to HGD/OAC. Guideline-recommended surveillance is effective, but is difficult to adhere to. Clinical predictors for those who are more likely to progress are yet to be defined.</p>\\n </section>\\n </div>\",\"PeriodicalId\":13625,\"journal\":{\"name\":\"Internal Medicine Journal\",\"volume\":\"54 11\",\"pages\":\"1867-1875\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/imj.16532\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Internal Medicine Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/imj.16532\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Internal Medicine Journal","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/imj.16532","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Outcomes of patients with Barrett's oesophagus with low-grade dysplasia undergoing endoscopic surveillance in a tertiary centre: a retrospective cohort study
Background and Aim
Barrett's oesophagus predisposes individuals to oesophageal adenocarcinoma (OAC), with the risk of progression to malignancy increasing with the degree of dysplasia, categorized as either low-grade dysplasia (LGD) or high-grade dysplasia (HGD). The reported incidence of progression to OAC in LGD ranges from 0.02% to 11.43% per annum. In patients with LGD, Australian guidelines recommend 6-monthly endoscopic surveillance. We aimed to describe the surveillance practices within a tertiary centre, and to determine the predictive value of surveillance as well as other risk factors for progression.
Methods
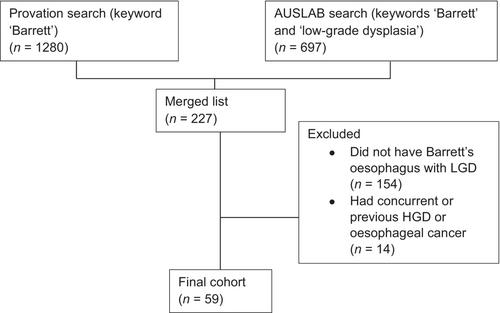
Endoscopy and pathology databases were searched over a 10-year period to collate all cases of Barrett's oesophagus with LGD. Medical records were reviewed to document patient factors and endoscopic and histologic details. Because follow-up times varied greatly, survival analysis techniques were employed.
Results
Fifty-nine patients were found to have LGD. Thirteen patients (22.0%) progressed to either HGD or OAC (10 (16.9%) and three (5.1%) respectively); the annual incidence rates of progression to HGD/OAC and OAC were 5.5% and 1.1% respectively. All patients who developed OAC had non-guideline-adherent surveillance. A Cox model found only two predictors of progression: (i) guideline-adherent surveillance, performed in 16 (27.1%), detected progression to HGD/OAC four times earlier than non-guideline-adherent surveillance (95% confidence interval (CI) = 1.3–12.3; P = 0.016). (ii) The detection of visible lesions at exit endoscopy independently predicted progression (hazard ratio = 6.5; 95% CI = 1.9–22.8; P = 0.003).
Conclusion
Barrett's oesophagus with LGD poses a significant risk of progression to HGD/OAC. Guideline-recommended surveillance is effective, but is difficult to adhere to. Clinical predictors for those who are more likely to progress are yet to be defined.
期刊介绍:
The Internal Medicine Journal is the official journal of the Adult Medicine Division of The Royal Australasian College of Physicians (RACP). Its purpose is to publish high-quality internationally competitive peer-reviewed original medical research, both laboratory and clinical, relating to the study and research of human disease. Papers will be considered from all areas of medical practice and science. The Journal also has a major role in continuing medical education and publishes review articles relevant to physician education.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


