{"title":"在日本,Atezolizumab 与 Durvalumab 作为广泛病变小细胞肺癌患者一线化疗联合疗法的成本效益比较。","authors":"Munenobu Kashiwa, Miho Tsukada, Ryo Matsushita","doi":"10.1007/s40261-024-01383-x","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND AND OBJECTIVE: Recent trials have shown that immune checkpoint inhibitors (ICIs), atezolizumab and durvalumab, in combination with chemotherapy, are effective in treating extensive-disease small-cell lung cancer (ED-SCLC). However, owing to the expensiveness of ICIs, monetary issues arise. The cost-effectiveness of ICI combination treatment with carboplatin plus etoposide (CE) as first-line therapy for patients with ED-SCLC was examined to aid public health policy in Japan.</p><p><strong>Methods: </strong>IMpower 133 and CASPIAN data were used to create a partitioned survival model. Medical expenses and quality-adjusted life years (QALYs) were considered. The analysis period, discount rate, and threshold were set at 20 years, 2%, and 15 million Japanese yen (JPY) [114,068 US dollars (USD)] per QALY, respectively. The incremental cost-effectiveness ratio (ICER) was calculated by gathering reasonable parameters from published reports and combining the costs and effects using parametric models. Monte Carlo simulations, scenario analysis, and one-way sensitivity analyses were employed to quantify uncertainty.</p><p><strong>Results: </strong>After comparing atezolizumab plus CE (ACE) and durvalumab plus CE (DCE) with CE, it was found that the ICERs exceeded the threshold at 35,048,299 JPY (266,527 USD) and 36,665,583 JPY (278,826 USD) per QALY, respectively. For one-way sensitivity and scenario assessments, the ICERs exceeded the threshold, even with considerably adjusted parameters. For the probabilistic sensitivity analyses, there was no probability that the ICER of the ICI combination treatment with chemotherapy would fall below the threshold.</p><p><strong>Conclusion: </strong>ACE and DCE were not cost-effective compared with CE as first-line therapy for ED-SCLC in Japan. Both these therapies exhibited high ICERs.</p>","PeriodicalId":10402,"journal":{"name":"Clinical Drug Investigation","volume":" ","pages":"749-759"},"PeriodicalIF":2.7000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499356/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative Cost-Effectiveness of Atezolizumab Versus Durvalumab as First-Line Combination Treatment with Chemotherapy for Patients with Extensive-Disease Small-Cell Lung Cancer in Japan.\",\"authors\":\"Munenobu Kashiwa, Miho Tsukada, Ryo Matsushita\",\"doi\":\"10.1007/s40261-024-01383-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND AND OBJECTIVE: Recent trials have shown that immune checkpoint inhibitors (ICIs), atezolizumab and durvalumab, in combination with chemotherapy, are effective in treating extensive-disease small-cell lung cancer (ED-SCLC). However, owing to the expensiveness of ICIs, monetary issues arise. The cost-effectiveness of ICI combination treatment with carboplatin plus etoposide (CE) as first-line therapy for patients with ED-SCLC was examined to aid public health policy in Japan.</p><p><strong>Methods: </strong>IMpower 133 and CASPIAN data were used to create a partitioned survival model. Medical expenses and quality-adjusted life years (QALYs) were considered. The analysis period, discount rate, and threshold were set at 20 years, 2%, and 15 million Japanese yen (JPY) [114,068 US dollars (USD)] per QALY, respectively. The incremental cost-effectiveness ratio (ICER) was calculated by gathering reasonable parameters from published reports and combining the costs and effects using parametric models. Monte Carlo simulations, scenario analysis, and one-way sensitivity analyses were employed to quantify uncertainty.</p><p><strong>Results: </strong>After comparing atezolizumab plus CE (ACE) and durvalumab plus CE (DCE) with CE, it was found that the ICERs exceeded the threshold at 35,048,299 JPY (266,527 USD) and 36,665,583 JPY (278,826 USD) per QALY, respectively. For one-way sensitivity and scenario assessments, the ICERs exceeded the threshold, even with considerably adjusted parameters. For the probabilistic sensitivity analyses, there was no probability that the ICER of the ICI combination treatment with chemotherapy would fall below the threshold.</p><p><strong>Conclusion: </strong>ACE and DCE were not cost-effective compared with CE as first-line therapy for ED-SCLC in Japan. Both these therapies exhibited high ICERs.</p>\",\"PeriodicalId\":10402,\"journal\":{\"name\":\"Clinical Drug Investigation\",\"volume\":\" \",\"pages\":\"749-759\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499356/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Drug Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40261-024-01383-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Drug Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40261-024-01383-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Comparative Cost-Effectiveness of Atezolizumab Versus Durvalumab as First-Line Combination Treatment with Chemotherapy for Patients with Extensive-Disease Small-Cell Lung Cancer in Japan.
BACKGROUND AND OBJECTIVE: Recent trials have shown that immune checkpoint inhibitors (ICIs), atezolizumab and durvalumab, in combination with chemotherapy, are effective in treating extensive-disease small-cell lung cancer (ED-SCLC). However, owing to the expensiveness of ICIs, monetary issues arise. The cost-effectiveness of ICI combination treatment with carboplatin plus etoposide (CE) as first-line therapy for patients with ED-SCLC was examined to aid public health policy in Japan.
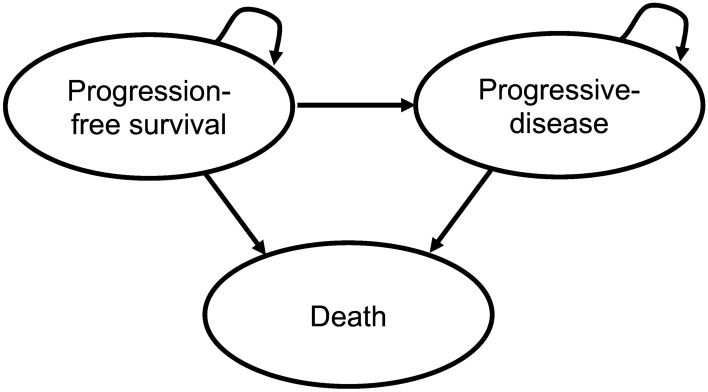
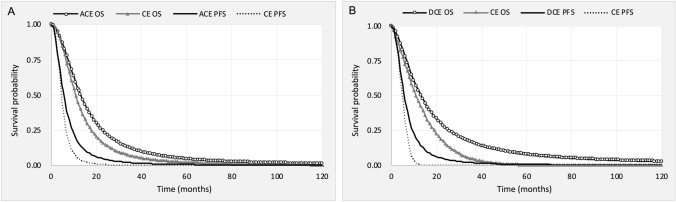
Methods: IMpower 133 and CASPIAN data were used to create a partitioned survival model. Medical expenses and quality-adjusted life years (QALYs) were considered. The analysis period, discount rate, and threshold were set at 20 years, 2%, and 15 million Japanese yen (JPY) [114,068 US dollars (USD)] per QALY, respectively. The incremental cost-effectiveness ratio (ICER) was calculated by gathering reasonable parameters from published reports and combining the costs and effects using parametric models. Monte Carlo simulations, scenario analysis, and one-way sensitivity analyses were employed to quantify uncertainty.
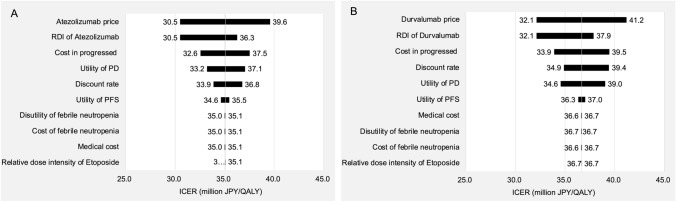
Results: After comparing atezolizumab plus CE (ACE) and durvalumab plus CE (DCE) with CE, it was found that the ICERs exceeded the threshold at 35,048,299 JPY (266,527 USD) and 36,665,583 JPY (278,826 USD) per QALY, respectively. For one-way sensitivity and scenario assessments, the ICERs exceeded the threshold, even with considerably adjusted parameters. For the probabilistic sensitivity analyses, there was no probability that the ICER of the ICI combination treatment with chemotherapy would fall below the threshold.
Conclusion: ACE and DCE were not cost-effective compared with CE as first-line therapy for ED-SCLC in Japan. Both these therapies exhibited high ICERs.
期刊介绍:
Clinical Drug Investigation provides rapid publication of original research covering all phases of clinical drug development and therapeutic use of drugs. The Journal includes:
-Clinical trials, outcomes research, clinical pharmacoeconomic studies and pharmacoepidemiology studies with a strong link to optimum prescribing practice for a drug or group of drugs.
-Clinical pharmacodynamic and clinical pharmacokinetic studies with a strong link to clinical practice.
-Pharmacodynamic and pharmacokinetic studies in healthy volunteers in which significant implications for clinical prescribing are discussed.
-Studies focusing on the application of drug delivery technology in healthcare.
-Short communications and case study reports that meet the above criteria will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Clinical Drug Investigation may be accompanied by plain language summaries to assist readers who have some knowledge, but non in-depth expertise in, the area to understand important medical advances.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


