Patricia Gina Lu, Zhi Ven Fong, Patrick T Hangge, Yu-Hui Chang, Elisabeth S Lim, Nabil Wasif, Patricia A Cronin, Chee-Chee Stucky
{"title":"2015年美国甲状腺协会指南更新后甲状腺叶切除术的使用差异。","authors":"Patricia Gina Lu, Zhi Ven Fong, Patrick T Hangge, Yu-Hui Chang, Elisabeth S Lim, Nabil Wasif, Patricia A Cronin, Chee-Chee Stucky","doi":"10.1530/EO-24-0010","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The 2015 American Thyroid Association (ATA) guidelines added thyroid lobectomy (TL) as the appropriate treatment for low-risk differentiated thyroid cancer (DTC). We aimed to investigate the population-level factors that influence the utilization of TL.</p><p><strong>Methods: </strong>The Surveillance, Epidemiology and End Results (SEER) database was queried for all DTC patients fitting low-risk criteria as defined by the ATA. Trends in total thyroidectomy (TT) and TL were identified using a Cochrane-Armitage test. Multivariable logistic regression identified patient and socioeconomic characteristics associated with TL, and difference-in-difference analysis was used to control for secular trends over time.</p><p><strong>Results: </strong>A total of 43,526 patients with low-risk DTC were identified in the SEER database; 39,411 pre-2015 and 4115 post-2015. After 2015, TT continued to outnumber TL (76.2% vs 23.8%), although the rate of TL increased significantly (11.6% to 23.8%, <i>P</i> < 0.001). However, difference-in-difference analysis found that age > 55 (OR 1.11, 95% CI 1.01-1.19, <i>P</i> < 0.001) and rurality (OR 1.16, 95% CI 1.05-1.28, <i>P</i> < 0.001) were independently associated with TT. TL was associated with T1 disease (OR 1.11, 95% CI 1.04-1.19, <i>P</i> = 0.001).</p><p><strong>Conclusion: </strong>Although the 2015 ATA guideline update led to an increase in TL for low-risk DTC, most patients still underwent TT. Age and neighborhood significantly impact the odds of receiving guideline-appropriate TL for low-risk DTC, especially for T2 disease.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"4 1","pages":"e240010"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11378144/pdf/","citationCount":"0","resultStr":"{\"title\":\"Differential utilization of thyroid lobectomy after the 2015 American Thyroid Association guideline update.\",\"authors\":\"Patricia Gina Lu, Zhi Ven Fong, Patrick T Hangge, Yu-Hui Chang, Elisabeth S Lim, Nabil Wasif, Patricia A Cronin, Chee-Chee Stucky\",\"doi\":\"10.1530/EO-24-0010\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The 2015 American Thyroid Association (ATA) guidelines added thyroid lobectomy (TL) as the appropriate treatment for low-risk differentiated thyroid cancer (DTC). We aimed to investigate the population-level factors that influence the utilization of TL.</p><p><strong>Methods: </strong>The Surveillance, Epidemiology and End Results (SEER) database was queried for all DTC patients fitting low-risk criteria as defined by the ATA. Trends in total thyroidectomy (TT) and TL were identified using a Cochrane-Armitage test. Multivariable logistic regression identified patient and socioeconomic characteristics associated with TL, and difference-in-difference analysis was used to control for secular trends over time.</p><p><strong>Results: </strong>A total of 43,526 patients with low-risk DTC were identified in the SEER database; 39,411 pre-2015 and 4115 post-2015. After 2015, TT continued to outnumber TL (76.2% vs 23.8%), although the rate of TL increased significantly (11.6% to 23.8%, <i>P</i> < 0.001). However, difference-in-difference analysis found that age > 55 (OR 1.11, 95% CI 1.01-1.19, <i>P</i> < 0.001) and rurality (OR 1.16, 95% CI 1.05-1.28, <i>P</i> < 0.001) were independently associated with TT. TL was associated with T1 disease (OR 1.11, 95% CI 1.04-1.19, <i>P</i> = 0.001).</p><p><strong>Conclusion: </strong>Although the 2015 ATA guideline update led to an increase in TL for low-risk DTC, most patients still underwent TT. Age and neighborhood significantly impact the odds of receiving guideline-appropriate TL for low-risk DTC, especially for T2 disease.</p>\",\"PeriodicalId\":72907,\"journal\":{\"name\":\"Endocrine oncology (Bristol, England)\",\"volume\":\"4 1\",\"pages\":\"e240010\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11378144/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine oncology (Bristol, England)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1530/EO-24-0010\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-24-0010","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:2015年美国甲状腺协会(ATA)指南增加了甲状腺叶切除术(TL)作为低风险分化型甲状腺癌(DTC)的适当治疗方法。我们旨在调查影响TL使用率的人群水平因素:我们在监测、流行病学和最终结果(SEER)数据库中查询了所有符合 ATA 定义的低风险标准的 DTC 患者。采用Cochrane-Armitage检验确定了甲状腺全切除术(TT)和TL的趋势。多变量逻辑回归确定了与TL相关的患者和社会经济特征,并使用差异分析控制了随时间变化的世俗趋势:SEER数据库共识别出43526名低风险DTC患者;2015年前为39411人,2015年后为4115人。2015 年后,TT 患者的数量继续超过 TL 患者(76.2% 对 23.8%),但 TL 的比例显著增加(11.6% 升至 23.8%,P < 0.001)。然而,差异分析发现,年龄大于 55 岁(OR 1.11,95% CI 1.01-1.19,P<0.001)和农村地区(OR 1.16,95% CI 1.05-1.28,P<0.001)与 TT 独立相关。TL与T1疾病相关(OR 1.11,95% CI 1.04-1.19,P = 0.001):尽管2015年ATA指南更新导致低风险DTC的TL增加,但大多数患者仍接受了TT。年龄和邻里关系对低风险 DTC(尤其是 T2 疾病)接受指南适当的 TL 的几率有很大影响。
Differential utilization of thyroid lobectomy after the 2015 American Thyroid Association guideline update.
Background: The 2015 American Thyroid Association (ATA) guidelines added thyroid lobectomy (TL) as the appropriate treatment for low-risk differentiated thyroid cancer (DTC). We aimed to investigate the population-level factors that influence the utilization of TL.
Methods: The Surveillance, Epidemiology and End Results (SEER) database was queried for all DTC patients fitting low-risk criteria as defined by the ATA. Trends in total thyroidectomy (TT) and TL were identified using a Cochrane-Armitage test. Multivariable logistic regression identified patient and socioeconomic characteristics associated with TL, and difference-in-difference analysis was used to control for secular trends over time.
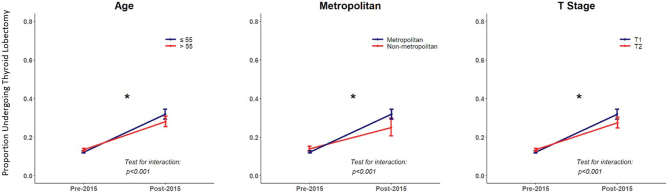
Results: A total of 43,526 patients with low-risk DTC were identified in the SEER database; 39,411 pre-2015 and 4115 post-2015. After 2015, TT continued to outnumber TL (76.2% vs 23.8%), although the rate of TL increased significantly (11.6% to 23.8%, P < 0.001). However, difference-in-difference analysis found that age > 55 (OR 1.11, 95% CI 1.01-1.19, P < 0.001) and rurality (OR 1.16, 95% CI 1.05-1.28, P < 0.001) were independently associated with TT. TL was associated with T1 disease (OR 1.11, 95% CI 1.04-1.19, P = 0.001).
Conclusion: Although the 2015 ATA guideline update led to an increase in TL for low-risk DTC, most patients still underwent TT. Age and neighborhood significantly impact the odds of receiving guideline-appropriate TL for low-risk DTC, especially for T2 disease.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


