Zoe McKinnell, Daniel Tuerff, Mustafa Hammudi, Colleen Hamilton, Martha Antonio, Ramesh Subrahmanyam, Joao Ascensao, Maneesh Rajiv Jain
{"title":"年轻人急性淋巴细胞白血病治疗结果的差异。","authors":"Zoe McKinnell, Daniel Tuerff, Mustafa Hammudi, Colleen Hamilton, Martha Antonio, Ramesh Subrahmanyam, Joao Ascensao, Maneesh Rajiv Jain","doi":"10.14740/jh1282","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Age is a strong prognostic factor in acute lymphocytic leukemia (ALL), with children doing better than adults with the same disease. One hypothesis for this age-based disparity is differences in treatment regimens. Optimizing care for adolescents and young adults (AYA) with ALL has not been well defined and disparities in care exist. We conducted a retrospective study of all veterans with ALL diagnosed between the ages of 18 and 45 since the year 2000 to evaluate disparities among prognostication methods, treatment regimens, and accrual to clinical trials with regard to age and race/ethnicity and how these factors influence overall survival.</p><p><strong>Methods: </strong>Electronic medical record data from the VA Informatics and Computing Infrastructure (VINCI) were used to identify 6,724 patients with an ICD-9 or 10 code for ALL. All patients were chart checked to confirm an ALL diagnosis between the ages of 18 and 45 and excluded if they were diagnosed before 2000, had childhood ALL, or if induction protocol was not recorded. A total of 252 patients were included in the final analysis. Multivariate analysis was performed with controls for age, ALL subtype (B, T, mixed phenotype), Ph status, cytogenetic risk (based on modified Medical Research Council-Eastern Cooperative Oncology Group (MRC-ECOG) study), obesity (body mass index (BMI) > 30), and race.</p><p><strong>Results: </strong>Patients treated with pediatric regimens, including pediatric-inspired regimens, have statistically significant (P = 0.009) survival gains, with a hazard ratio (HR) of 0.52 after controlling for age, obesity, ALL subtype, cytogenetic risk and race. White patients had significantly improved OS compared to people of color (HR 0.57, P = 0.02) after controlling for the aforementioned covariates. Black patients were far less likely (23%) to receive a transplant than non-Black patients (46%). Only 7% of patients were treated on a clinical trial.</p><p><strong>Conclusions: </strong>These data demonstrate that treatment with a pediatric regimen significantly improves overall survival in patients up to the age of 45 and suggests ongoing shortcomings in treatment for young adults with ALL, especially 30 to 45 years old, including persistently high use of adult induction regimens, low rates of referral to clinical trials, and significant racial disparities in bone marrow transplants for Black patients.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"13 4","pages":"150-157"},"PeriodicalIF":1.3000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11379050/pdf/","citationCount":"0","resultStr":"{\"title\":\"Disparities in Acute Lymphocytic Leukemia Outcomes Among Young Adults.\",\"authors\":\"Zoe McKinnell, Daniel Tuerff, Mustafa Hammudi, Colleen Hamilton, Martha Antonio, Ramesh Subrahmanyam, Joao Ascensao, Maneesh Rajiv Jain\",\"doi\":\"10.14740/jh1282\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Age is a strong prognostic factor in acute lymphocytic leukemia (ALL), with children doing better than adults with the same disease. One hypothesis for this age-based disparity is differences in treatment regimens. Optimizing care for adolescents and young adults (AYA) with ALL has not been well defined and disparities in care exist. We conducted a retrospective study of all veterans with ALL diagnosed between the ages of 18 and 45 since the year 2000 to evaluate disparities among prognostication methods, treatment regimens, and accrual to clinical trials with regard to age and race/ethnicity and how these factors influence overall survival.</p><p><strong>Methods: </strong>Electronic medical record data from the VA Informatics and Computing Infrastructure (VINCI) were used to identify 6,724 patients with an ICD-9 or 10 code for ALL. All patients were chart checked to confirm an ALL diagnosis between the ages of 18 and 45 and excluded if they were diagnosed before 2000, had childhood ALL, or if induction protocol was not recorded. A total of 252 patients were included in the final analysis. Multivariate analysis was performed with controls for age, ALL subtype (B, T, mixed phenotype), Ph status, cytogenetic risk (based on modified Medical Research Council-Eastern Cooperative Oncology Group (MRC-ECOG) study), obesity (body mass index (BMI) > 30), and race.</p><p><strong>Results: </strong>Patients treated with pediatric regimens, including pediatric-inspired regimens, have statistically significant (P = 0.009) survival gains, with a hazard ratio (HR) of 0.52 after controlling for age, obesity, ALL subtype, cytogenetic risk and race. White patients had significantly improved OS compared to people of color (HR 0.57, P = 0.02) after controlling for the aforementioned covariates. Black patients were far less likely (23%) to receive a transplant than non-Black patients (46%). Only 7% of patients were treated on a clinical trial.</p><p><strong>Conclusions: </strong>These data demonstrate that treatment with a pediatric regimen significantly improves overall survival in patients up to the age of 45 and suggests ongoing shortcomings in treatment for young adults with ALL, especially 30 to 45 years old, including persistently high use of adult induction regimens, low rates of referral to clinical trials, and significant racial disparities in bone marrow transplants for Black patients.</p>\",\"PeriodicalId\":15964,\"journal\":{\"name\":\"Journal of hematology\",\"volume\":\"13 4\",\"pages\":\"150-157\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11379050/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jh1282\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh1282","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/15 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Disparities in Acute Lymphocytic Leukemia Outcomes Among Young Adults.
Background: Age is a strong prognostic factor in acute lymphocytic leukemia (ALL), with children doing better than adults with the same disease. One hypothesis for this age-based disparity is differences in treatment regimens. Optimizing care for adolescents and young adults (AYA) with ALL has not been well defined and disparities in care exist. We conducted a retrospective study of all veterans with ALL diagnosed between the ages of 18 and 45 since the year 2000 to evaluate disparities among prognostication methods, treatment regimens, and accrual to clinical trials with regard to age and race/ethnicity and how these factors influence overall survival.
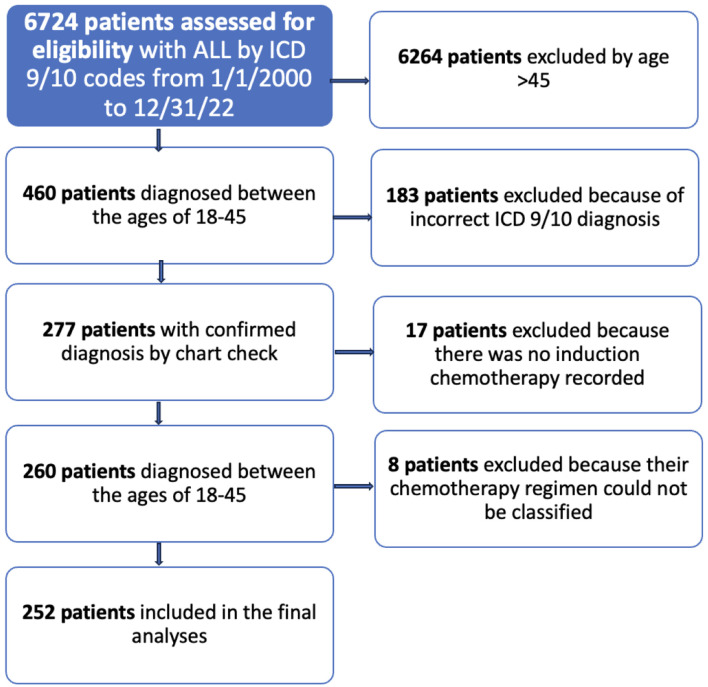
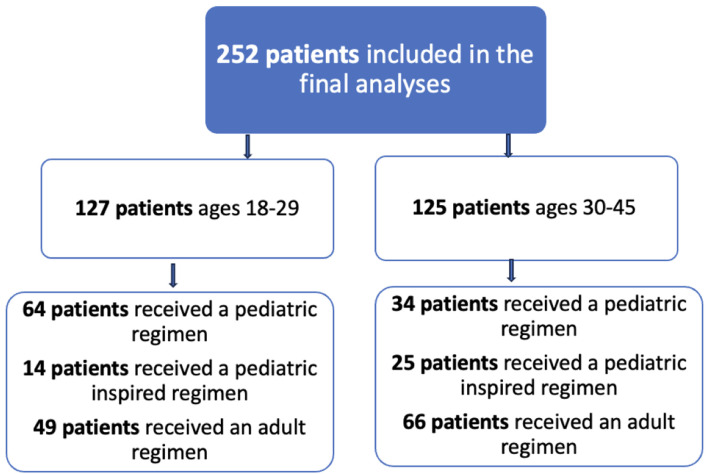
Methods: Electronic medical record data from the VA Informatics and Computing Infrastructure (VINCI) were used to identify 6,724 patients with an ICD-9 or 10 code for ALL. All patients were chart checked to confirm an ALL diagnosis between the ages of 18 and 45 and excluded if they were diagnosed before 2000, had childhood ALL, or if induction protocol was not recorded. A total of 252 patients were included in the final analysis. Multivariate analysis was performed with controls for age, ALL subtype (B, T, mixed phenotype), Ph status, cytogenetic risk (based on modified Medical Research Council-Eastern Cooperative Oncology Group (MRC-ECOG) study), obesity (body mass index (BMI) > 30), and race.
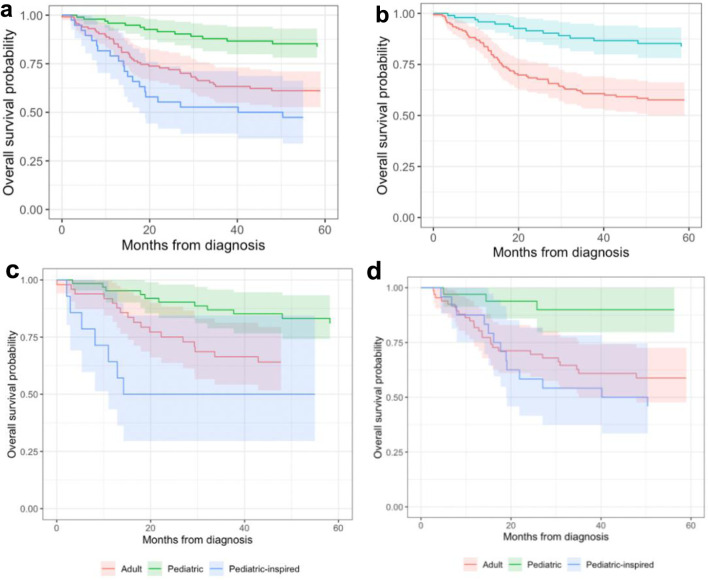
Results: Patients treated with pediatric regimens, including pediatric-inspired regimens, have statistically significant (P = 0.009) survival gains, with a hazard ratio (HR) of 0.52 after controlling for age, obesity, ALL subtype, cytogenetic risk and race. White patients had significantly improved OS compared to people of color (HR 0.57, P = 0.02) after controlling for the aforementioned covariates. Black patients were far less likely (23%) to receive a transplant than non-Black patients (46%). Only 7% of patients were treated on a clinical trial.
Conclusions: These data demonstrate that treatment with a pediatric regimen significantly improves overall survival in patients up to the age of 45 and suggests ongoing shortcomings in treatment for young adults with ALL, especially 30 to 45 years old, including persistently high use of adult induction regimens, low rates of referral to clinical trials, and significant racial disparities in bone marrow transplants for Black patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


