Karolina A. Klucznik, Thomas Ravkilde, Simon Skouboe, Ditte S. Møller, Steffen B. Hokland, Paul Keall, Simon Buus, Lise Bentzen, Per R. Poulsen
{"title":"量化前列腺和盆腔淋巴结的平移和旋转运动对高风险前列腺放疗造成的剂量扰动。","authors":"Karolina A. Klucznik, Thomas Ravkilde, Simon Skouboe, Ditte S. Møller, Steffen B. Hokland, Paul Keall, Simon Buus, Lise Bentzen, Per R. Poulsen","doi":"10.1002/mp.17366","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Radiotherapy of the prostate and the pelvic lymph nodes (LN) is a part of the standard of care treatment for high-risk prostate cancer. The independent translational and rotational (i.e., six-degrees-of-freedom, [6DoF]) motion of the prostate and LN target during and between fractions can perturb the dose distribution. However, no standard dose reconstruction method accounting for differential 6DoF target motion is available.</p>\n </section>\n \n <section>\n \n <h3> Purpose</h3>\n \n <p>We present a framework for monitoring motion-induced dose perturbations for two independently moving target volumes in 6DoF. The framework was used to determine the dose perturbation for the prostate and the LN target caused by differential 6DoF motion for a cohort of high-risk prostate cancer patients. As a potential first step toward real-time dose-guided high-risk prostate radiotherapy, we furthermore investigated if the dose reconstruction was fast enough for real-time application for both targets.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Twenty high-risk prostate cancer patients were treated with 3-arc volumetric modulated arc therapy (VMAT). Kilovoltage intrafraction monitoring (KIM) with triggered kilovoltage (kV) images acquired every 3 throughout 7–10 fractions per patient was used for retrospective 6DoF intrafraction prostate motion estimation. The 6DoF interfraction LN motion was determined from a pelvic bone match between the planning CT and a post-treatment cone beam CT (CBCT). Using the retrospectively extracted motion, real-time 6DoF motion-including dose reconstruction was simulated using the in-house developed software DoseTracker. A data stream with the 6DoF target positions and linac parameters was broadcasted at a 3-Hz frequency to DoseTracker. In a continuous loop, DoseTracker calculated the target dose increments including the specified motion and, for comparison, without motion. The motion-induced change in D<sub>99.5%</sub> for the prostate CTV (ΔD<sub>99.5%</sub>) and in D<sub>98%</sub> for the LN CTV (ΔD<sub>98%</sub>) was calculated using the final cumulative dose of each fraction and averaged over all imaged fractions. The real-time reconstructed dose distribution of DoseTracker was benchmarked against a clinical treatment planning system (TPS) and it was investigated whether the calculation speed was fast enough to keep up with the incoming data stream.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Translational motion was largest in cranio-caudal (CC) direction (prostate: [-5.9, +8.4] mm; LN: [-9.9; +11.0] mm) and anterior–posterior (AP) direction (prostate:[-5.6; +6.9] mm; LN: [-9.6; +11.0] mm). The pitch was the largest rotation (prostate: [-22.5; +25.2] deg; LN: [-3.9; +5.5] deg). The prostate CTV ΔD<sub>99.5%</sub> was [-16.2; +2.5]% for single fractions and [-3.0; +1.7]% when averaged over all imaged fractions. The LN CTV ΔD<sub>98%</sub> was [-19.8; +1.2]% for single fractions and [-3.1; +0.9]% after averaging. Mean (Standard deviation) absolute dose errors in DoseTracker of 107.8% (Std: 1.9%) for the prostate and 105.5% (Std:1.4%) for the LN were corrected during dose reconstruction by automatically calculated normalization factors. It resulted in accurate calculation of the motion-induced dose errors with relative differences between DoseTracker and TPS dose calculations of -0.1% (Std: 0.5%) (prostate CTV ΔD<sub>99.5%</sub>) and -0.2% (Std: 0.5%) (LN CTV ΔD<sub>98%</sub>). The DoseTracker calculation was fast enough to keep up with the incoming inputs for all but two out of 107 184 dose calculations.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Using the developed framework for dose perturbation monitoring, we found that the differential 6DoF target motion caused substantial dose perturbation for individual fractions, which largely averaged out after several fractions. The framework was shown to provide reliable dose calculations and a sufficiently high-dose reconstruction speed to be applicable in real-time.</p>\n </section>\n </div>","PeriodicalId":18384,"journal":{"name":"Medical physics","volume":"51 11","pages":"8423-8433"},"PeriodicalIF":3.2000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mp.17366","citationCount":"0","resultStr":"{\"title\":\"Quantifying dose perturbations in high-risk prostate radiotherapy due to translational and rotational motion of prostate and pelvic lymph nodes\",\"authors\":\"Karolina A. Klucznik, Thomas Ravkilde, Simon Skouboe, Ditte S. Møller, Steffen B. Hokland, Paul Keall, Simon Buus, Lise Bentzen, Per R. Poulsen\",\"doi\":\"10.1002/mp.17366\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Radiotherapy of the prostate and the pelvic lymph nodes (LN) is a part of the standard of care treatment for high-risk prostate cancer. The independent translational and rotational (i.e., six-degrees-of-freedom, [6DoF]) motion of the prostate and LN target during and between fractions can perturb the dose distribution. However, no standard dose reconstruction method accounting for differential 6DoF target motion is available.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Purpose</h3>\\n \\n <p>We present a framework for monitoring motion-induced dose perturbations for two independently moving target volumes in 6DoF. The framework was used to determine the dose perturbation for the prostate and the LN target caused by differential 6DoF motion for a cohort of high-risk prostate cancer patients. As a potential first step toward real-time dose-guided high-risk prostate radiotherapy, we furthermore investigated if the dose reconstruction was fast enough for real-time application for both targets.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Twenty high-risk prostate cancer patients were treated with 3-arc volumetric modulated arc therapy (VMAT). Kilovoltage intrafraction monitoring (KIM) with triggered kilovoltage (kV) images acquired every 3 throughout 7–10 fractions per patient was used for retrospective 6DoF intrafraction prostate motion estimation. The 6DoF interfraction LN motion was determined from a pelvic bone match between the planning CT and a post-treatment cone beam CT (CBCT). Using the retrospectively extracted motion, real-time 6DoF motion-including dose reconstruction was simulated using the in-house developed software DoseTracker. A data stream with the 6DoF target positions and linac parameters was broadcasted at a 3-Hz frequency to DoseTracker. In a continuous loop, DoseTracker calculated the target dose increments including the specified motion and, for comparison, without motion. The motion-induced change in D<sub>99.5%</sub> for the prostate CTV (ΔD<sub>99.5%</sub>) and in D<sub>98%</sub> for the LN CTV (ΔD<sub>98%</sub>) was calculated using the final cumulative dose of each fraction and averaged over all imaged fractions. The real-time reconstructed dose distribution of DoseTracker was benchmarked against a clinical treatment planning system (TPS) and it was investigated whether the calculation speed was fast enough to keep up with the incoming data stream.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Translational motion was largest in cranio-caudal (CC) direction (prostate: [-5.9, +8.4] mm; LN: [-9.9; +11.0] mm) and anterior–posterior (AP) direction (prostate:[-5.6; +6.9] mm; LN: [-9.6; +11.0] mm). The pitch was the largest rotation (prostate: [-22.5; +25.2] deg; LN: [-3.9; +5.5] deg). The prostate CTV ΔD<sub>99.5%</sub> was [-16.2; +2.5]% for single fractions and [-3.0; +1.7]% when averaged over all imaged fractions. The LN CTV ΔD<sub>98%</sub> was [-19.8; +1.2]% for single fractions and [-3.1; +0.9]% after averaging. Mean (Standard deviation) absolute dose errors in DoseTracker of 107.8% (Std: 1.9%) for the prostate and 105.5% (Std:1.4%) for the LN were corrected during dose reconstruction by automatically calculated normalization factors. It resulted in accurate calculation of the motion-induced dose errors with relative differences between DoseTracker and TPS dose calculations of -0.1% (Std: 0.5%) (prostate CTV ΔD<sub>99.5%</sub>) and -0.2% (Std: 0.5%) (LN CTV ΔD<sub>98%</sub>). The DoseTracker calculation was fast enough to keep up with the incoming inputs for all but two out of 107 184 dose calculations.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Using the developed framework for dose perturbation monitoring, we found that the differential 6DoF target motion caused substantial dose perturbation for individual fractions, which largely averaged out after several fractions. The framework was shown to provide reliable dose calculations and a sufficiently high-dose reconstruction speed to be applicable in real-time.</p>\\n </section>\\n </div>\",\"PeriodicalId\":18384,\"journal\":{\"name\":\"Medical physics\",\"volume\":\"51 11\",\"pages\":\"8423-8433\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mp.17366\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical physics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/mp.17366\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical physics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/mp.17366","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Quantifying dose perturbations in high-risk prostate radiotherapy due to translational and rotational motion of prostate and pelvic lymph nodes
Background
Radiotherapy of the prostate and the pelvic lymph nodes (LN) is a part of the standard of care treatment for high-risk prostate cancer. The independent translational and rotational (i.e., six-degrees-of-freedom, [6DoF]) motion of the prostate and LN target during and between fractions can perturb the dose distribution. However, no standard dose reconstruction method accounting for differential 6DoF target motion is available.
Purpose
We present a framework for monitoring motion-induced dose perturbations for two independently moving target volumes in 6DoF. The framework was used to determine the dose perturbation for the prostate and the LN target caused by differential 6DoF motion for a cohort of high-risk prostate cancer patients. As a potential first step toward real-time dose-guided high-risk prostate radiotherapy, we furthermore investigated if the dose reconstruction was fast enough for real-time application for both targets.
Methods
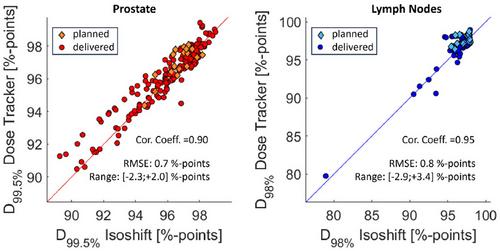
Twenty high-risk prostate cancer patients were treated with 3-arc volumetric modulated arc therapy (VMAT). Kilovoltage intrafraction monitoring (KIM) with triggered kilovoltage (kV) images acquired every 3 throughout 7–10 fractions per patient was used for retrospective 6DoF intrafraction prostate motion estimation. The 6DoF interfraction LN motion was determined from a pelvic bone match between the planning CT and a post-treatment cone beam CT (CBCT). Using the retrospectively extracted motion, real-time 6DoF motion-including dose reconstruction was simulated using the in-house developed software DoseTracker. A data stream with the 6DoF target positions and linac parameters was broadcasted at a 3-Hz frequency to DoseTracker. In a continuous loop, DoseTracker calculated the target dose increments including the specified motion and, for comparison, without motion. The motion-induced change in D99.5% for the prostate CTV (ΔD99.5%) and in D98% for the LN CTV (ΔD98%) was calculated using the final cumulative dose of each fraction and averaged over all imaged fractions. The real-time reconstructed dose distribution of DoseTracker was benchmarked against a clinical treatment planning system (TPS) and it was investigated whether the calculation speed was fast enough to keep up with the incoming data stream.
Results
Translational motion was largest in cranio-caudal (CC) direction (prostate: [-5.9, +8.4] mm; LN: [-9.9; +11.0] mm) and anterior–posterior (AP) direction (prostate:[-5.6; +6.9] mm; LN: [-9.6; +11.0] mm). The pitch was the largest rotation (prostate: [-22.5; +25.2] deg; LN: [-3.9; +5.5] deg). The prostate CTV ΔD99.5% was [-16.2; +2.5]% for single fractions and [-3.0; +1.7]% when averaged over all imaged fractions. The LN CTV ΔD98% was [-19.8; +1.2]% for single fractions and [-3.1; +0.9]% after averaging. Mean (Standard deviation) absolute dose errors in DoseTracker of 107.8% (Std: 1.9%) for the prostate and 105.5% (Std:1.4%) for the LN were corrected during dose reconstruction by automatically calculated normalization factors. It resulted in accurate calculation of the motion-induced dose errors with relative differences between DoseTracker and TPS dose calculations of -0.1% (Std: 0.5%) (prostate CTV ΔD99.5%) and -0.2% (Std: 0.5%) (LN CTV ΔD98%). The DoseTracker calculation was fast enough to keep up with the incoming inputs for all but two out of 107 184 dose calculations.
Conclusion
Using the developed framework for dose perturbation monitoring, we found that the differential 6DoF target motion caused substantial dose perturbation for individual fractions, which largely averaged out after several fractions. The framework was shown to provide reliable dose calculations and a sufficiently high-dose reconstruction speed to be applicable in real-time.
期刊介绍:
Medical Physics publishes original, high impact physics, imaging science, and engineering research that advances patient diagnosis and therapy through contributions in 1) Basic science developments with high potential for clinical translation 2) Clinical applications of cutting edge engineering and physics innovations 3) Broadly applicable and innovative clinical physics developments
Medical Physics is a journal of global scope and reach. By publishing in Medical Physics your research will reach an international, multidisciplinary audience including practicing medical physicists as well as physics- and engineering based translational scientists. We work closely with authors of promising articles to improve their quality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


