Mikko Kosunen, Jarno Ruotsalainen, Alvar Kallio, Roope Metsä, Paavo Raittinen, Leena Lehmus, Maarit J Korhonen, Timo Purmonen
{"title":"多发性骨髓瘤确诊后头 5 年及生命末期的医疗资源利用率和相关费用:芬兰全国多发性骨髓瘤患者队列研究》。","authors":"Mikko Kosunen, Jarno Ruotsalainen, Alvar Kallio, Roope Metsä, Paavo Raittinen, Leena Lehmus, Maarit J Korhonen, Timo Purmonen","doi":"10.1007/s41669-024-00524-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The burden associated with the treatment of patients with multiple myeloma (MM) is expected to increase due to the aging population. Thus, policymakers and clinicians need a holistic view of the healthcare resource use (HCRU) and costs associated with MM and its treatment for informed decision making. However, nationwide information on HCRU and costs due to MM is scarce in Finland. The aim of this study was to determine healthcare resource utilization, patterns of service use and associated costs among Finnish patients with MM during the first 5 years from their first diagnosis and at end of life.</p><p><strong>Methods: </strong>Data on patients newly diagnosed with MM and receiving treatment for it in Finland in 2015-2019 was sourced from comprehensive nationwide registers. Data on all-cause and MM-specific HCRU including inpatient stays, outpatient visits and contacts, emergency care visits and home care were obtained separately from specialized and primary care registers. HCRU costs were assessed by multiplying the numbers of primary and specialized care contacts by respective national unit costs. For reimbursed outpatient medication and reimbursed sick leave, data on actual costs were collected. All registry data were linked via unique personal identifiers, and follow-up time was up to 5 years.</p><p><strong>Results: </strong>Altogether, 1615 patients were included in the analyses. In the 5-year follow-up period, patients had on average 96 healthcare contacts per patient-year (PPY) and the mean all-cause healthcare costs were €46,000 PPY. Around 47% of these costs originated from reimbursed outpatient medication and the rest from healthcare contacts. Over half (60%) of the contacts occurred in primary care but most of the costs were associated with specialized care. Additionally, 29% of contacts were MM-specific, but they were responsible for 58% of the costs. The HCRU was highest during the first year after diagnosis, levelled off during the follow-up and then increased significantly during the last year of patients' lives. The number of all-cause healthcare contacts PPY was approximately 53% higher, and the respective costs were 5% higher during the last year of a patient's life when compared with the first year after diagnosis. During the last 12 months (N = 417) and 6 months (N = 505) of life and during palliative care (N = 145), the most common healthcare contact was home care.</p><p><strong>Conclusions: </strong>During active treatment, MM is primarily treated in the specialized care setting, with outpatient medication and visits to specialized care being the main cost drivers. These results can be utilized to estimate the need for care and expected costs over time due to MM and in health economic evaluations concerning MM.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"57-68"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717749/pdf/","citationCount":"0","resultStr":"{\"title\":\"Healthcare Resource Utilization and Associated Costs During the First 5 Years After Diagnosis and at the End of Life: A Nationwide Cohort Study of Patients with Multiple Myeloma in Finland.\",\"authors\":\"Mikko Kosunen, Jarno Ruotsalainen, Alvar Kallio, Roope Metsä, Paavo Raittinen, Leena Lehmus, Maarit J Korhonen, Timo Purmonen\",\"doi\":\"10.1007/s41669-024-00524-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The burden associated with the treatment of patients with multiple myeloma (MM) is expected to increase due to the aging population. Thus, policymakers and clinicians need a holistic view of the healthcare resource use (HCRU) and costs associated with MM and its treatment for informed decision making. However, nationwide information on HCRU and costs due to MM is scarce in Finland. The aim of this study was to determine healthcare resource utilization, patterns of service use and associated costs among Finnish patients with MM during the first 5 years from their first diagnosis and at end of life.</p><p><strong>Methods: </strong>Data on patients newly diagnosed with MM and receiving treatment for it in Finland in 2015-2019 was sourced from comprehensive nationwide registers. Data on all-cause and MM-specific HCRU including inpatient stays, outpatient visits and contacts, emergency care visits and home care were obtained separately from specialized and primary care registers. HCRU costs were assessed by multiplying the numbers of primary and specialized care contacts by respective national unit costs. For reimbursed outpatient medication and reimbursed sick leave, data on actual costs were collected. All registry data were linked via unique personal identifiers, and follow-up time was up to 5 years.</p><p><strong>Results: </strong>Altogether, 1615 patients were included in the analyses. In the 5-year follow-up period, patients had on average 96 healthcare contacts per patient-year (PPY) and the mean all-cause healthcare costs were €46,000 PPY. Around 47% of these costs originated from reimbursed outpatient medication and the rest from healthcare contacts. Over half (60%) of the contacts occurred in primary care but most of the costs were associated with specialized care. Additionally, 29% of contacts were MM-specific, but they were responsible for 58% of the costs. The HCRU was highest during the first year after diagnosis, levelled off during the follow-up and then increased significantly during the last year of patients' lives. The number of all-cause healthcare contacts PPY was approximately 53% higher, and the respective costs were 5% higher during the last year of a patient's life when compared with the first year after diagnosis. During the last 12 months (N = 417) and 6 months (N = 505) of life and during palliative care (N = 145), the most common healthcare contact was home care.</p><p><strong>Conclusions: </strong>During active treatment, MM is primarily treated in the specialized care setting, with outpatient medication and visits to specialized care being the main cost drivers. These results can be utilized to estimate the need for care and expected costs over time due to MM and in health economic evaluations concerning MM.</p>\",\"PeriodicalId\":19770,\"journal\":{\"name\":\"PharmacoEconomics Open\",\"volume\":\" \",\"pages\":\"57-68\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717749/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s41669-024-00524-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-024-00524-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
Healthcare Resource Utilization and Associated Costs During the First 5 Years After Diagnosis and at the End of Life: A Nationwide Cohort Study of Patients with Multiple Myeloma in Finland.
Background: The burden associated with the treatment of patients with multiple myeloma (MM) is expected to increase due to the aging population. Thus, policymakers and clinicians need a holistic view of the healthcare resource use (HCRU) and costs associated with MM and its treatment for informed decision making. However, nationwide information on HCRU and costs due to MM is scarce in Finland. The aim of this study was to determine healthcare resource utilization, patterns of service use and associated costs among Finnish patients with MM during the first 5 years from their first diagnosis and at end of life.
Methods: Data on patients newly diagnosed with MM and receiving treatment for it in Finland in 2015-2019 was sourced from comprehensive nationwide registers. Data on all-cause and MM-specific HCRU including inpatient stays, outpatient visits and contacts, emergency care visits and home care were obtained separately from specialized and primary care registers. HCRU costs were assessed by multiplying the numbers of primary and specialized care contacts by respective national unit costs. For reimbursed outpatient medication and reimbursed sick leave, data on actual costs were collected. All registry data were linked via unique personal identifiers, and follow-up time was up to 5 years.
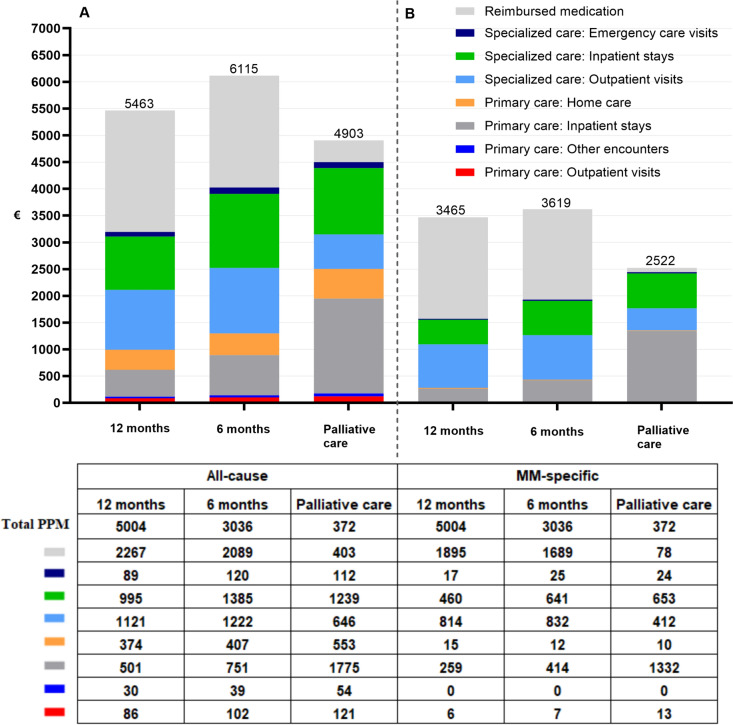
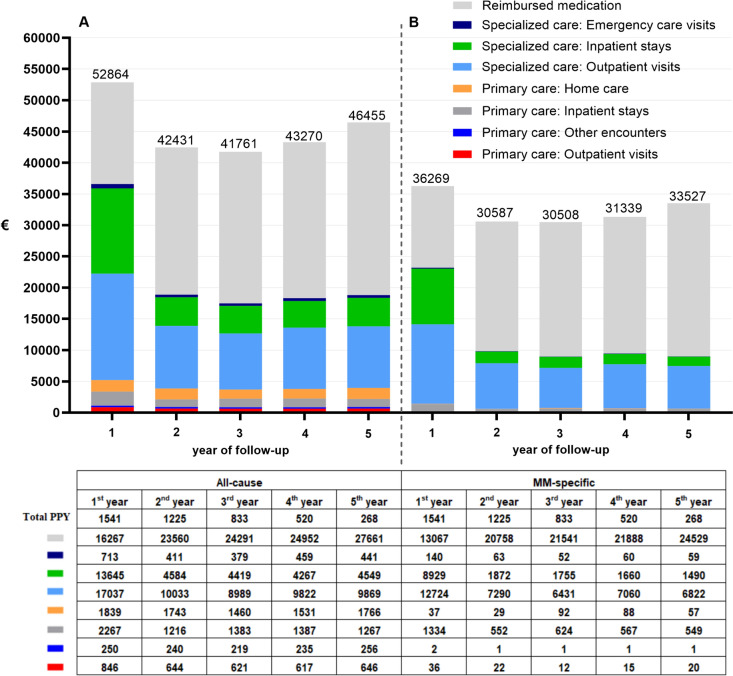
Results: Altogether, 1615 patients were included in the analyses. In the 5-year follow-up period, patients had on average 96 healthcare contacts per patient-year (PPY) and the mean all-cause healthcare costs were €46,000 PPY. Around 47% of these costs originated from reimbursed outpatient medication and the rest from healthcare contacts. Over half (60%) of the contacts occurred in primary care but most of the costs were associated with specialized care. Additionally, 29% of contacts were MM-specific, but they were responsible for 58% of the costs. The HCRU was highest during the first year after diagnosis, levelled off during the follow-up and then increased significantly during the last year of patients' lives. The number of all-cause healthcare contacts PPY was approximately 53% higher, and the respective costs were 5% higher during the last year of a patient's life when compared with the first year after diagnosis. During the last 12 months (N = 417) and 6 months (N = 505) of life and during palliative care (N = 145), the most common healthcare contact was home care.
Conclusions: During active treatment, MM is primarily treated in the specialized care setting, with outpatient medication and visits to specialized care being the main cost drivers. These results can be utilized to estimate the need for care and expected costs over time due to MM and in health economic evaluations concerning MM.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


