Maryza Graham, Thomas Tran, Changxu Zhang, Michelle Sam, Andrew Daley, Kathy Jackson, Chuan Kok Lim
{"title":"2023 年底和 2024 年初,维多利亚州的两个主要检测实验室检测到肺炎支原体呼吸道感染病例上升。","authors":"Maryza Graham, Thomas Tran, Changxu Zhang, Michelle Sam, Andrew Daley, Kathy Jackson, Chuan Kok Lim","doi":"10.5694/mja2.52433","DOIUrl":null,"url":null,"abstract":"<p>In November 2023, the World Health Organization noted that the numbers of outpatient consultations and hospital admissions for children with pneumonia caused by <i>Mycoplasma pneumoniae</i> had increased in China since May 2023.<span><sup>1</sup></span> In Denmark, a surge in <i>M. pneumoniae</i> infections since October 2023 was reported, most in children or adolescents, but the impact on hospital capacity was limited; 446 of 3195 people (14%), primarily adults, required hospitalisation.<span><sup>2</sup></span></p><p>The most frequent manifestation of <i>M. pneumoniae</i> infection in school-aged children, pneumonia, is generally mild. However, people of all ages can require hospitalisation because of severe community-acquired pneumonia (CAP) or extrapulmonary manifestations (including haemolysis and central nervous system disease).<span><sup>3</sup></span> <i>M. pneumoniae</i> is the most frequently detected bacterial pathogen in children hospitalised with CAP.<span><sup>4</sup></span> Infections are most frequent during summer and early autumn, but can develop at any time of year. The cumulative attack rate in families approaches 90%, and immunity is not long lasting.<span><sup>2</sup></span> <i>M. pneumoniae</i> is resistant to β-lactam antibiotics, the mainstay of the empiric treatment of CAP. Recommended treatments for <i>M. pneumoniae</i> include macrolide, tetracycline, and fluoroquinolone antibiotics, the prescribing of which requires clinical suspicion of this infection.</p><p>We reviewed the results of polymerase chain reaction (PCR) testing for <i>M. pneumoniae</i> in the laboratory information systems of the Victorian Infectious Diseases Reference Laboratory (VIDRL; 1 January 2016 – 30 April 2024) and the Royal Children's Hospital (RCH; 1 January 2018 – 31 January 2024). At VIDRL, only samples for which <i>M. pneumoniae</i> testing is specifically requested by the ordering clinician are tested (targeted testing). At RCH, targeted testing was undertaken prior to 2020; from January 2020, a syndromic multiplex PCR panel was used that included <i>M. pneumoniae</i> targets (Respiratory Pathogens 16-well REF 20620; AusDiagnostics), and all samples submitted for respiratory pathogen testing were therefore tested for <i>M. pneumoniae</i> (untargeted testing). Reporting by VIDRL of information on currently circulating pathogens, including outbreak or transmission investigations, is approved by the Office for Research Ethics and Governance of the Royal Melbourne Hospital (QA2022085); the analysis of RCH data for public health surveillance has local governance approval from the hospital legal services and human research ethics committee.</p><p>The <i>M. pneumoniae</i> positivity rate at RCH was 4% (five of 124 samples) in 2018 and 8% (12 of 148 samples) in 2019 (targeted testing). At VIDRL, 5.9% (five of 85 samples) were positive in 2016; during 2016–2022 the positivity rate was 1.3% (15 of 1148 samples; targeted testing). Three of 14 837 RCH and VIDRL samples were PCR-positive during July 2020 – December 2022; during January–October 2023, the positivity rate was 0.2% at RCH (21 of 8873 samples; untargeted testing) and 1.5% at VIDRL (11 of 734 samples; targeted testing). <i>M. pneumoniae</i> positivity rates began to rise in October 2023, reaching their highest levels since 2016: 6.8% at RCH (43 of 627 samples; untargeted testing) in January 2024, and 21.6% at VIDRL (33 of 153 samples; targeted testing) in January 2024 and 19.7% (57 of 289; targeted testing) in April 2024 (Box 1; Supporting Information).</p><p>During August 2023 – January 2024, 80 people were PCR-positive for <i>M. pneumoniae</i> at RCH (Box 2). None required intensive care, and the proportions of positive sample types indicating invasive disease (eg, cerebrospinal fluid, lower respiratory tract samples) did not increase (data not shown). A total of 4251 nasopharyngeal swabs or aspirates, ten throat swabs, 47 sputum samples, 142 bronchoalveolar lavage samples, and 78 miscellaneous sample types were tested at RCH during this period; 695 upper respiratory tract swabs, 146 sputum samples, 23 bronchoalveolar lavage samples, 12 cerebrospinal fluid samples, and 16 miscellaneous sample types were tested at VIDRL.</p><p>In conclusion, we detected a rise in the number of <i>M. pneumoniae</i> infections in Victoria beginning in October 2023. This rise was later than rises reported in other parts of the world, delayed until after the relaxation of COVID-19-related restrictions in Victoria. The higher rates have continued until April 2024, the proportion of positive test results reaching the highest sustained level since 2016. No signals for greater disease severity during the peak were detected. A higher index of suspicion for this pathogen is needed, as specific requesting for <i>M. pneumoniae</i> testing may be required.</p><p>Open access publishing facilitated by Monash University, as part of the Wiley – Monash University agreement via the Council of Australian University Librarians.</p><p>No relevant disclosures.</p><p>We had full access to all of the data (including statistical reports and tables) in the study. Individual-level data are not publicly available for sharing.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 8","pages":"436-437"},"PeriodicalIF":6.7000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52433","citationCount":"0","resultStr":"{\"title\":\"A rise in Mycoplasma pneumoniae respiratory infections in Victoria in late 2023 and early 2024 detected at two major testing laboratories\",\"authors\":\"Maryza Graham, Thomas Tran, Changxu Zhang, Michelle Sam, Andrew Daley, Kathy Jackson, Chuan Kok Lim\",\"doi\":\"10.5694/mja2.52433\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In November 2023, the World Health Organization noted that the numbers of outpatient consultations and hospital admissions for children with pneumonia caused by <i>Mycoplasma pneumoniae</i> had increased in China since May 2023.<span><sup>1</sup></span> In Denmark, a surge in <i>M. pneumoniae</i> infections since October 2023 was reported, most in children or adolescents, but the impact on hospital capacity was limited; 446 of 3195 people (14%), primarily adults, required hospitalisation.<span><sup>2</sup></span></p><p>The most frequent manifestation of <i>M. pneumoniae</i> infection in school-aged children, pneumonia, is generally mild. However, people of all ages can require hospitalisation because of severe community-acquired pneumonia (CAP) or extrapulmonary manifestations (including haemolysis and central nervous system disease).<span><sup>3</sup></span> <i>M. pneumoniae</i> is the most frequently detected bacterial pathogen in children hospitalised with CAP.<span><sup>4</sup></span> Infections are most frequent during summer and early autumn, but can develop at any time of year. The cumulative attack rate in families approaches 90%, and immunity is not long lasting.<span><sup>2</sup></span> <i>M. pneumoniae</i> is resistant to β-lactam antibiotics, the mainstay of the empiric treatment of CAP. Recommended treatments for <i>M. pneumoniae</i> include macrolide, tetracycline, and fluoroquinolone antibiotics, the prescribing of which requires clinical suspicion of this infection.</p><p>We reviewed the results of polymerase chain reaction (PCR) testing for <i>M. pneumoniae</i> in the laboratory information systems of the Victorian Infectious Diseases Reference Laboratory (VIDRL; 1 January 2016 – 30 April 2024) and the Royal Children's Hospital (RCH; 1 January 2018 – 31 January 2024). At VIDRL, only samples for which <i>M. pneumoniae</i> testing is specifically requested by the ordering clinician are tested (targeted testing). At RCH, targeted testing was undertaken prior to 2020; from January 2020, a syndromic multiplex PCR panel was used that included <i>M. pneumoniae</i> targets (Respiratory Pathogens 16-well REF 20620; AusDiagnostics), and all samples submitted for respiratory pathogen testing were therefore tested for <i>M. pneumoniae</i> (untargeted testing). Reporting by VIDRL of information on currently circulating pathogens, including outbreak or transmission investigations, is approved by the Office for Research Ethics and Governance of the Royal Melbourne Hospital (QA2022085); the analysis of RCH data for public health surveillance has local governance approval from the hospital legal services and human research ethics committee.</p><p>The <i>M. pneumoniae</i> positivity rate at RCH was 4% (five of 124 samples) in 2018 and 8% (12 of 148 samples) in 2019 (targeted testing). At VIDRL, 5.9% (five of 85 samples) were positive in 2016; during 2016–2022 the positivity rate was 1.3% (15 of 1148 samples; targeted testing). Three of 14 837 RCH and VIDRL samples were PCR-positive during July 2020 – December 2022; during January–October 2023, the positivity rate was 0.2% at RCH (21 of 8873 samples; untargeted testing) and 1.5% at VIDRL (11 of 734 samples; targeted testing). <i>M. pneumoniae</i> positivity rates began to rise in October 2023, reaching their highest levels since 2016: 6.8% at RCH (43 of 627 samples; untargeted testing) in January 2024, and 21.6% at VIDRL (33 of 153 samples; targeted testing) in January 2024 and 19.7% (57 of 289; targeted testing) in April 2024 (Box 1; Supporting Information).</p><p>During August 2023 – January 2024, 80 people were PCR-positive for <i>M. pneumoniae</i> at RCH (Box 2). None required intensive care, and the proportions of positive sample types indicating invasive disease (eg, cerebrospinal fluid, lower respiratory tract samples) did not increase (data not shown). A total of 4251 nasopharyngeal swabs or aspirates, ten throat swabs, 47 sputum samples, 142 bronchoalveolar lavage samples, and 78 miscellaneous sample types were tested at RCH during this period; 695 upper respiratory tract swabs, 146 sputum samples, 23 bronchoalveolar lavage samples, 12 cerebrospinal fluid samples, and 16 miscellaneous sample types were tested at VIDRL.</p><p>In conclusion, we detected a rise in the number of <i>M. pneumoniae</i> infections in Victoria beginning in October 2023. This rise was later than rises reported in other parts of the world, delayed until after the relaxation of COVID-19-related restrictions in Victoria. The higher rates have continued until April 2024, the proportion of positive test results reaching the highest sustained level since 2016. No signals for greater disease severity during the peak were detected. A higher index of suspicion for this pathogen is needed, as specific requesting for <i>M. pneumoniae</i> testing may be required.</p><p>Open access publishing facilitated by Monash University, as part of the Wiley – Monash University agreement via the Council of Australian University Librarians.</p><p>No relevant disclosures.</p><p>We had full access to all of the data (including statistical reports and tables) in the study. Individual-level data are not publicly available for sharing.</p>\",\"PeriodicalId\":18214,\"journal\":{\"name\":\"Medical Journal of Australia\",\"volume\":\"221 8\",\"pages\":\"436-437\"},\"PeriodicalIF\":6.7000,\"publicationDate\":\"2024-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52433\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical Journal of Australia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52433\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52433","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
A rise in Mycoplasma pneumoniae respiratory infections in Victoria in late 2023 and early 2024 detected at two major testing laboratories
In November 2023, the World Health Organization noted that the numbers of outpatient consultations and hospital admissions for children with pneumonia caused by Mycoplasma pneumoniae had increased in China since May 2023.1 In Denmark, a surge in M. pneumoniae infections since October 2023 was reported, most in children or adolescents, but the impact on hospital capacity was limited; 446 of 3195 people (14%), primarily adults, required hospitalisation.2
The most frequent manifestation of M. pneumoniae infection in school-aged children, pneumonia, is generally mild. However, people of all ages can require hospitalisation because of severe community-acquired pneumonia (CAP) or extrapulmonary manifestations (including haemolysis and central nervous system disease).3M. pneumoniae is the most frequently detected bacterial pathogen in children hospitalised with CAP.4 Infections are most frequent during summer and early autumn, but can develop at any time of year. The cumulative attack rate in families approaches 90%, and immunity is not long lasting.2M. pneumoniae is resistant to β-lactam antibiotics, the mainstay of the empiric treatment of CAP. Recommended treatments for M. pneumoniae include macrolide, tetracycline, and fluoroquinolone antibiotics, the prescribing of which requires clinical suspicion of this infection.
We reviewed the results of polymerase chain reaction (PCR) testing for M. pneumoniae in the laboratory information systems of the Victorian Infectious Diseases Reference Laboratory (VIDRL; 1 January 2016 – 30 April 2024) and the Royal Children's Hospital (RCH; 1 January 2018 – 31 January 2024). At VIDRL, only samples for which M. pneumoniae testing is specifically requested by the ordering clinician are tested (targeted testing). At RCH, targeted testing was undertaken prior to 2020; from January 2020, a syndromic multiplex PCR panel was used that included M. pneumoniae targets (Respiratory Pathogens 16-well REF 20620; AusDiagnostics), and all samples submitted for respiratory pathogen testing were therefore tested for M. pneumoniae (untargeted testing). Reporting by VIDRL of information on currently circulating pathogens, including outbreak or transmission investigations, is approved by the Office for Research Ethics and Governance of the Royal Melbourne Hospital (QA2022085); the analysis of RCH data for public health surveillance has local governance approval from the hospital legal services and human research ethics committee.
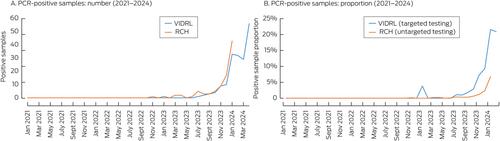
The M. pneumoniae positivity rate at RCH was 4% (five of 124 samples) in 2018 and 8% (12 of 148 samples) in 2019 (targeted testing). At VIDRL, 5.9% (five of 85 samples) were positive in 2016; during 2016–2022 the positivity rate was 1.3% (15 of 1148 samples; targeted testing). Three of 14 837 RCH and VIDRL samples were PCR-positive during July 2020 – December 2022; during January–October 2023, the positivity rate was 0.2% at RCH (21 of 8873 samples; untargeted testing) and 1.5% at VIDRL (11 of 734 samples; targeted testing). M. pneumoniae positivity rates began to rise in October 2023, reaching their highest levels since 2016: 6.8% at RCH (43 of 627 samples; untargeted testing) in January 2024, and 21.6% at VIDRL (33 of 153 samples; targeted testing) in January 2024 and 19.7% (57 of 289; targeted testing) in April 2024 (Box 1; Supporting Information).
During August 2023 – January 2024, 80 people were PCR-positive for M. pneumoniae at RCH (Box 2). None required intensive care, and the proportions of positive sample types indicating invasive disease (eg, cerebrospinal fluid, lower respiratory tract samples) did not increase (data not shown). A total of 4251 nasopharyngeal swabs or aspirates, ten throat swabs, 47 sputum samples, 142 bronchoalveolar lavage samples, and 78 miscellaneous sample types were tested at RCH during this period; 695 upper respiratory tract swabs, 146 sputum samples, 23 bronchoalveolar lavage samples, 12 cerebrospinal fluid samples, and 16 miscellaneous sample types were tested at VIDRL.
In conclusion, we detected a rise in the number of M. pneumoniae infections in Victoria beginning in October 2023. This rise was later than rises reported in other parts of the world, delayed until after the relaxation of COVID-19-related restrictions in Victoria. The higher rates have continued until April 2024, the proportion of positive test results reaching the highest sustained level since 2016. No signals for greater disease severity during the peak were detected. A higher index of suspicion for this pathogen is needed, as specific requesting for M. pneumoniae testing may be required.
Open access publishing facilitated by Monash University, as part of the Wiley – Monash University agreement via the Council of Australian University Librarians.
No relevant disclosures.
We had full access to all of the data (including statistical reports and tables) in the study. Individual-level data are not publicly available for sharing.
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


