Kalyan Mansukhbhai Shekhda, Vladislav Zlatkin, Bernard Khoo, Eleni Armeni
{"title":"妊娠滋养细胞疾病导致的甲亢:妊娠滋养细胞疾病引起的甲状腺毒症:妊娠甲状腺毒症治疗中尚未满足的需求。","authors":"Kalyan Mansukhbhai Shekhda, Vladislav Zlatkin, Bernard Khoo, Eleni Armeni","doi":"10.1155/2024/5318871","DOIUrl":null,"url":null,"abstract":"<p><p>Thyrotoxicosis during pregnancy is rare but can have severe adverse consequences for the mother or foetus if left undiagnosed and untreated. It can be caused by an underlying thyroid disease or develop as gestational transient thyrotoxicosis. Molar pregnancy stands out as a pathological condition characterized by abnormal trophoblastic cell growth, which can manifest in benign or malignant forms, and is diagnosed with a disproportionate elevation of <i>β</i>-hCG (beta-human chorionic gonadotrophin) and specific features on ultrasonography including absent sac and large multicystic or honeycomb appearance. A pronounced increase in <i>β</i>-hCG levels can trigger hyperthyroidism, due to the structural resemblance between <i>β</i>-hCG and thyroid-stimulating hormone (TSH), although the thyrotrophic effects of <i>β</i>-hCG could vary between patients diagnosed with gestational trophoblastic disease (GTD). In this report, we present two cases (Patient 1: 43 years, Patient 2: 31 years) who came to emergency department following a history of vaginal spotting, palpitations, and hyperemesis. In both patients, blood tests indicated disproportionately elevated <i>β</i>-hCG levels along with high levels of Free T4 (FT4) and Free T3 (FT3), as well as suppressed TSH levels. Ultrasonography showed nonviable products of conception with large multicystic hemorrhagic lesions and empty gestational sacs, thereby confirming GTD. The Burch-Wartofsky Point Scale scores were 20 and 15 points, respectively, suggesting that they were less likely to be in thyroid storm at presentation. Antithyroid medications were administered, followed by evacuation of the products of conception. Postoperatively, their thyroid function was normalized. These cases underscore the importance of ruling out thyroid storm, monitoring thyroid function, and treating hyperthyroidism appropriately before undergoing surgical treatment. It is also important to consider the variability in the thyrotrophic effects of <i>β</i>-hCG among individuals diagnosed with GTD. In addition to monitoring free thyroid hormone levels, it is crucial to consider clinical symptoms to effectively manage such cases.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2024 ","pages":"5318871"},"PeriodicalIF":0.9000,"publicationDate":"2024-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11377108/pdf/","citationCount":"0","resultStr":"{\"title\":\"Thyrotoxicosis due to Gestational Trophoblastic Disease: Unmet Needs in the Management of Gestational Thyrotoxicosis.\",\"authors\":\"Kalyan Mansukhbhai Shekhda, Vladislav Zlatkin, Bernard Khoo, Eleni Armeni\",\"doi\":\"10.1155/2024/5318871\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Thyrotoxicosis during pregnancy is rare but can have severe adverse consequences for the mother or foetus if left undiagnosed and untreated. It can be caused by an underlying thyroid disease or develop as gestational transient thyrotoxicosis. Molar pregnancy stands out as a pathological condition characterized by abnormal trophoblastic cell growth, which can manifest in benign or malignant forms, and is diagnosed with a disproportionate elevation of <i>β</i>-hCG (beta-human chorionic gonadotrophin) and specific features on ultrasonography including absent sac and large multicystic or honeycomb appearance. A pronounced increase in <i>β</i>-hCG levels can trigger hyperthyroidism, due to the structural resemblance between <i>β</i>-hCG and thyroid-stimulating hormone (TSH), although the thyrotrophic effects of <i>β</i>-hCG could vary between patients diagnosed with gestational trophoblastic disease (GTD). In this report, we present two cases (Patient 1: 43 years, Patient 2: 31 years) who came to emergency department following a history of vaginal spotting, palpitations, and hyperemesis. In both patients, blood tests indicated disproportionately elevated <i>β</i>-hCG levels along with high levels of Free T4 (FT4) and Free T3 (FT3), as well as suppressed TSH levels. Ultrasonography showed nonviable products of conception with large multicystic hemorrhagic lesions and empty gestational sacs, thereby confirming GTD. The Burch-Wartofsky Point Scale scores were 20 and 15 points, respectively, suggesting that they were less likely to be in thyroid storm at presentation. Antithyroid medications were administered, followed by evacuation of the products of conception. Postoperatively, their thyroid function was normalized. These cases underscore the importance of ruling out thyroid storm, monitoring thyroid function, and treating hyperthyroidism appropriately before undergoing surgical treatment. It is also important to consider the variability in the thyrotrophic effects of <i>β</i>-hCG among individuals diagnosed with GTD. In addition to monitoring free thyroid hormone levels, it is crucial to consider clinical symptoms to effectively manage such cases.</p>\",\"PeriodicalId\":9621,\"journal\":{\"name\":\"Case Reports in Endocrinology\",\"volume\":\"2024 \",\"pages\":\"5318871\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11377108/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/5318871\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/5318871","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Thyrotoxicosis due to Gestational Trophoblastic Disease: Unmet Needs in the Management of Gestational Thyrotoxicosis.
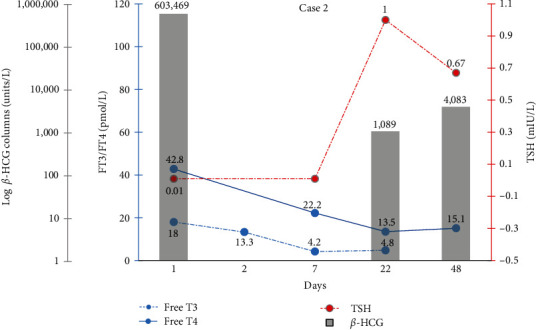
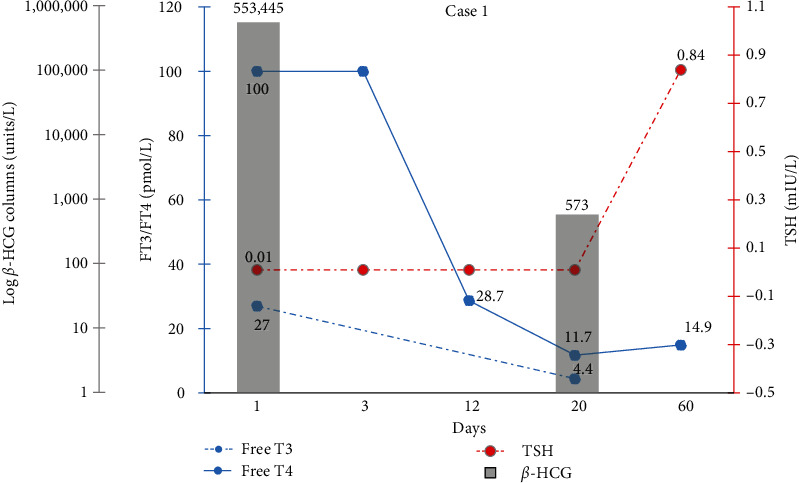
Thyrotoxicosis during pregnancy is rare but can have severe adverse consequences for the mother or foetus if left undiagnosed and untreated. It can be caused by an underlying thyroid disease or develop as gestational transient thyrotoxicosis. Molar pregnancy stands out as a pathological condition characterized by abnormal trophoblastic cell growth, which can manifest in benign or malignant forms, and is diagnosed with a disproportionate elevation of β-hCG (beta-human chorionic gonadotrophin) and specific features on ultrasonography including absent sac and large multicystic or honeycomb appearance. A pronounced increase in β-hCG levels can trigger hyperthyroidism, due to the structural resemblance between β-hCG and thyroid-stimulating hormone (TSH), although the thyrotrophic effects of β-hCG could vary between patients diagnosed with gestational trophoblastic disease (GTD). In this report, we present two cases (Patient 1: 43 years, Patient 2: 31 years) who came to emergency department following a history of vaginal spotting, palpitations, and hyperemesis. In both patients, blood tests indicated disproportionately elevated β-hCG levels along with high levels of Free T4 (FT4) and Free T3 (FT3), as well as suppressed TSH levels. Ultrasonography showed nonviable products of conception with large multicystic hemorrhagic lesions and empty gestational sacs, thereby confirming GTD. The Burch-Wartofsky Point Scale scores were 20 and 15 points, respectively, suggesting that they were less likely to be in thyroid storm at presentation. Antithyroid medications were administered, followed by evacuation of the products of conception. Postoperatively, their thyroid function was normalized. These cases underscore the importance of ruling out thyroid storm, monitoring thyroid function, and treating hyperthyroidism appropriately before undergoing surgical treatment. It is also important to consider the variability in the thyrotrophic effects of β-hCG among individuals diagnosed with GTD. In addition to monitoring free thyroid hormone levels, it is crucial to consider clinical symptoms to effectively manage such cases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


