Annabel S van Lieshout, Lisanne J H Smits, Julie M L Sijmons, Susan van Dieren, Stefan E van Oostendorp, Pieter J Tanis, Jurriaan B Tuynman
{"title":"早期直肠癌初次全直肠系膜切除术 (TME) 与局部切除术后再行全直肠系膜切除术的短期疗效对比:基于人群的倾向匹配研究。","authors":"Annabel S van Lieshout, Lisanne J H Smits, Julie M L Sijmons, Susan van Dieren, Stefan E van Oostendorp, Pieter J Tanis, Jurriaan B Tuynman","doi":"10.1093/bjsopen/zrae103","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Colorectal cancer screening programmes have led to a shift towards early-stage colorectal cancer, which, in selected cases, can be treated using local excision. However, local excision followed by completion total mesorectal excision (two-stage approach) may be associated with less favourable outcomes than primary total mesorectal excision (one-stage approach). The aim of this population study was to determine the distribution of treatment strategies for early rectal cancer in the Netherlands and to compare the short-term outcomes of primary total mesorectal excision with those of local excision followed by completion total mesorectal excision.</p><p><strong>Methods: </strong>Short-term data for patients with cT1-2 N0xM0 rectal cancer who underwent local excision only, primary total mesorectal excision, or local excision followed by completion total mesorectal excision between 2012 and 2020 in the Netherlands were collected from the Dutch Colorectal Audit. Patients were categorized according to treatment groups and logistic regressions were performed after multiple imputation and propensity score matching. The primary outcome was the end-ostomy rate.</p><p><strong>Results: </strong>From 2015 to 2020, the proportion for the two-stage approach increased from 22.3% to 43.9%. After matching, 1062 patients were included. The end-ostomy rate was 16.8% for the primary total mesorectal excision group versus 29.6% for the local excision followed by completion total mesorectal excision group (P < 0.001). The primary total mesorectal excision group had a higher re-intervention rate than the local excision followed by completion total mesorectal excision group (16.7% versus 11.8%; P = 0.048). No differences were observed with regard to complications, conversion, diverting ostomies, radical resections, readmissions, and death.</p><p><strong>Conclusion: </strong>This study shows that, over time, cT1-2 rectal cancer has increasingly been treated using the two-stage approach. However, local excision followed by completion total mesorectal excision seems to be associated with an elevated end-ostomy rate. It is important that clinicians and patients are aware of this risk during shared decision-making.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"8 5","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11375580/pdf/","citationCount":"0","resultStr":"{\"title\":\"Short-term outcomes after primary total mesorectal excision (TME) versus local excision followed by completion TME for early rectal cancer: population-based propensity-matched study.\",\"authors\":\"Annabel S van Lieshout, Lisanne J H Smits, Julie M L Sijmons, Susan van Dieren, Stefan E van Oostendorp, Pieter J Tanis, Jurriaan B Tuynman\",\"doi\":\"10.1093/bjsopen/zrae103\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Colorectal cancer screening programmes have led to a shift towards early-stage colorectal cancer, which, in selected cases, can be treated using local excision. However, local excision followed by completion total mesorectal excision (two-stage approach) may be associated with less favourable outcomes than primary total mesorectal excision (one-stage approach). The aim of this population study was to determine the distribution of treatment strategies for early rectal cancer in the Netherlands and to compare the short-term outcomes of primary total mesorectal excision with those of local excision followed by completion total mesorectal excision.</p><p><strong>Methods: </strong>Short-term data for patients with cT1-2 N0xM0 rectal cancer who underwent local excision only, primary total mesorectal excision, or local excision followed by completion total mesorectal excision between 2012 and 2020 in the Netherlands were collected from the Dutch Colorectal Audit. Patients were categorized according to treatment groups and logistic regressions were performed after multiple imputation and propensity score matching. The primary outcome was the end-ostomy rate.</p><p><strong>Results: </strong>From 2015 to 2020, the proportion for the two-stage approach increased from 22.3% to 43.9%. After matching, 1062 patients were included. The end-ostomy rate was 16.8% for the primary total mesorectal excision group versus 29.6% for the local excision followed by completion total mesorectal excision group (P < 0.001). The primary total mesorectal excision group had a higher re-intervention rate than the local excision followed by completion total mesorectal excision group (16.7% versus 11.8%; P = 0.048). No differences were observed with regard to complications, conversion, diverting ostomies, radical resections, readmissions, and death.</p><p><strong>Conclusion: </strong>This study shows that, over time, cT1-2 rectal cancer has increasingly been treated using the two-stage approach. However, local excision followed by completion total mesorectal excision seems to be associated with an elevated end-ostomy rate. It is important that clinicians and patients are aware of this risk during shared decision-making.</p>\",\"PeriodicalId\":9028,\"journal\":{\"name\":\"BJS Open\",\"volume\":\"8 5\",\"pages\":\"\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11375580/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJS Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/bjsopen/zrae103\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zrae103","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
Short-term outcomes after primary total mesorectal excision (TME) versus local excision followed by completion TME for early rectal cancer: population-based propensity-matched study.
Background: Colorectal cancer screening programmes have led to a shift towards early-stage colorectal cancer, which, in selected cases, can be treated using local excision. However, local excision followed by completion total mesorectal excision (two-stage approach) may be associated with less favourable outcomes than primary total mesorectal excision (one-stage approach). The aim of this population study was to determine the distribution of treatment strategies for early rectal cancer in the Netherlands and to compare the short-term outcomes of primary total mesorectal excision with those of local excision followed by completion total mesorectal excision.
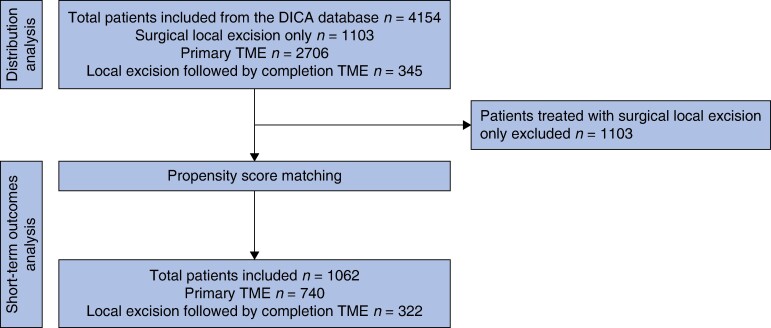
Methods: Short-term data for patients with cT1-2 N0xM0 rectal cancer who underwent local excision only, primary total mesorectal excision, or local excision followed by completion total mesorectal excision between 2012 and 2020 in the Netherlands were collected from the Dutch Colorectal Audit. Patients were categorized according to treatment groups and logistic regressions were performed after multiple imputation and propensity score matching. The primary outcome was the end-ostomy rate.
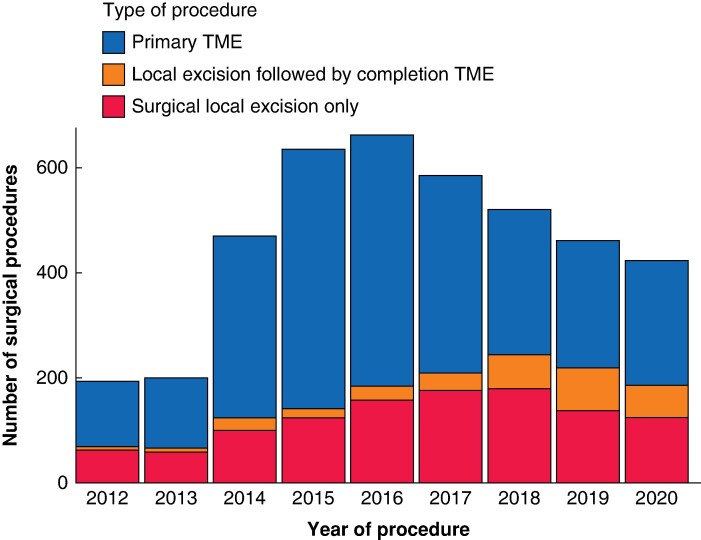
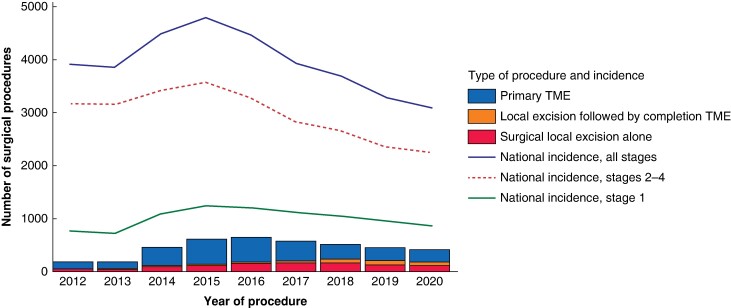
Results: From 2015 to 2020, the proportion for the two-stage approach increased from 22.3% to 43.9%. After matching, 1062 patients were included. The end-ostomy rate was 16.8% for the primary total mesorectal excision group versus 29.6% for the local excision followed by completion total mesorectal excision group (P < 0.001). The primary total mesorectal excision group had a higher re-intervention rate than the local excision followed by completion total mesorectal excision group (16.7% versus 11.8%; P = 0.048). No differences were observed with regard to complications, conversion, diverting ostomies, radical resections, readmissions, and death.
Conclusion: This study shows that, over time, cT1-2 rectal cancer has increasingly been treated using the two-stage approach. However, local excision followed by completion total mesorectal excision seems to be associated with an elevated end-ostomy rate. It is important that clinicians and patients are aware of this risk during shared decision-making.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


