Felipe Eltit, Qiong Wang, Naomi Jung, Sheryl Munshan, Dennis Xie, Samuel Xu, Doris Liang, Bita Mojtahedzadeh, Danmei Liu, Raphaële Charest-Morin, Eva Corey, Lawrence D True, Colm Morrissey, Rizhi Wang, Michael E Cox
{"title":"硬化性前列腺癌骨转移:扭曲的编织骨病变。","authors":"Felipe Eltit, Qiong Wang, Naomi Jung, Sheryl Munshan, Dennis Xie, Samuel Xu, Doris Liang, Bita Mojtahedzadeh, Danmei Liu, Raphaële Charest-Morin, Eva Corey, Lawrence D True, Colm Morrissey, Rizhi Wang, Michael E Cox","doi":"10.1093/jbmrpl/ziae091","DOIUrl":null,"url":null,"abstract":"<p><p>Bone metastases are the most severe and prevalent consequences of prostate cancer (PC), affecting more than 80% of patients with advanced PC. PCBMs generate pain, pathological fractures, and paralysis. As modern therapies increase survival, more patients are suffering from these catastrophic consequences. Radiographically, PCBMs are predominantly osteosclerotic, but the mechanisms of abnormal bone formation and how this pathological increase in bone density is related to fractures are unclear. In this study, we conducted a comprehensive analysis on a cohort of 76 cadaveric PCBM specimens and 12 cancer-free specimens as controls. We used micro-computed tomography to determine 3D organization and quantify bone characteristics, quantitative backscattering electron microscopy to characterize mineral content and details in bone structure, nanoindentation to determine mechanical properties, and histological and immunohistochemical analysis of bone structure and composition. We define 4 PCBM phenotypes: osteolytic, mixed lytic-sclerotic, and 2 subgroups of osteosclerotic lesions-those with residual trabeculae, and others without residual trabeculae. The osteosclerotic lesions are characterized by the presence of abnormal bone accumulated on trabeculae surfaces and within intertrabecular spaces. This abnormal bone is characterized by higher lacunae density, abnormal lacunae morphology, and irregular lacunae orientation. However, mineral content, hardness, and elastic modulus at micron-scale were indistinguishable between this irregular bone and residual trabeculae. The collagen matrix of this abnormal bone presents with irregular organization and a prominent collagen III composition. These characteristics suggest that osteosclerotic PCBMs initiate new bone deposition as woven bone; however, the lack of subsequent bone remodeling, absence of lamellar bone deposition on its surface, and presence of collagen III distinguish this pathologic matrix from conventional woven bone. Although the mineralized matrix retains normal bone hardness and stiffness properties, the lack of fibril anisotropy presents a compromised trabecular structure, which may have clinical implications.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"8 10","pages":"ziae091"},"PeriodicalIF":2.4000,"publicationDate":"2024-07-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11365963/pdf/","citationCount":"0","resultStr":"{\"title\":\"Sclerotic prostate cancer bone metastasis: woven bone lesions with a twist.\",\"authors\":\"Felipe Eltit, Qiong Wang, Naomi Jung, Sheryl Munshan, Dennis Xie, Samuel Xu, Doris Liang, Bita Mojtahedzadeh, Danmei Liu, Raphaële Charest-Morin, Eva Corey, Lawrence D True, Colm Morrissey, Rizhi Wang, Michael E Cox\",\"doi\":\"10.1093/jbmrpl/ziae091\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Bone metastases are the most severe and prevalent consequences of prostate cancer (PC), affecting more than 80% of patients with advanced PC. PCBMs generate pain, pathological fractures, and paralysis. As modern therapies increase survival, more patients are suffering from these catastrophic consequences. Radiographically, PCBMs are predominantly osteosclerotic, but the mechanisms of abnormal bone formation and how this pathological increase in bone density is related to fractures are unclear. In this study, we conducted a comprehensive analysis on a cohort of 76 cadaveric PCBM specimens and 12 cancer-free specimens as controls. We used micro-computed tomography to determine 3D organization and quantify bone characteristics, quantitative backscattering electron microscopy to characterize mineral content and details in bone structure, nanoindentation to determine mechanical properties, and histological and immunohistochemical analysis of bone structure and composition. We define 4 PCBM phenotypes: osteolytic, mixed lytic-sclerotic, and 2 subgroups of osteosclerotic lesions-those with residual trabeculae, and others without residual trabeculae. The osteosclerotic lesions are characterized by the presence of abnormal bone accumulated on trabeculae surfaces and within intertrabecular spaces. This abnormal bone is characterized by higher lacunae density, abnormal lacunae morphology, and irregular lacunae orientation. However, mineral content, hardness, and elastic modulus at micron-scale were indistinguishable between this irregular bone and residual trabeculae. The collagen matrix of this abnormal bone presents with irregular organization and a prominent collagen III composition. These characteristics suggest that osteosclerotic PCBMs initiate new bone deposition as woven bone; however, the lack of subsequent bone remodeling, absence of lamellar bone deposition on its surface, and presence of collagen III distinguish this pathologic matrix from conventional woven bone. Although the mineralized matrix retains normal bone hardness and stiffness properties, the lack of fibril anisotropy presents a compromised trabecular structure, which may have clinical implications.</p>\",\"PeriodicalId\":14611,\"journal\":{\"name\":\"JBMR Plus\",\"volume\":\"8 10\",\"pages\":\"ziae091\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-07-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11365963/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBMR Plus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jbmrpl/ziae091\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
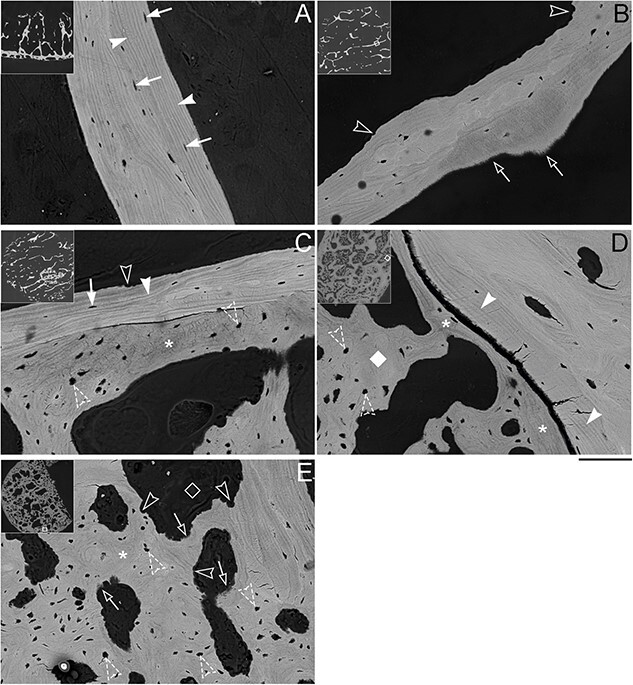
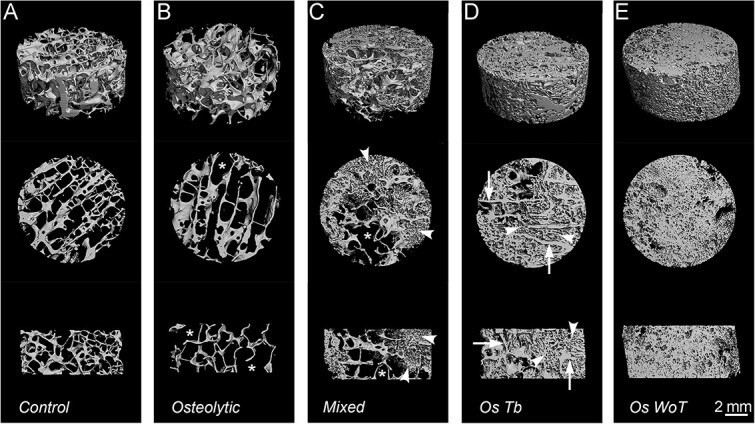
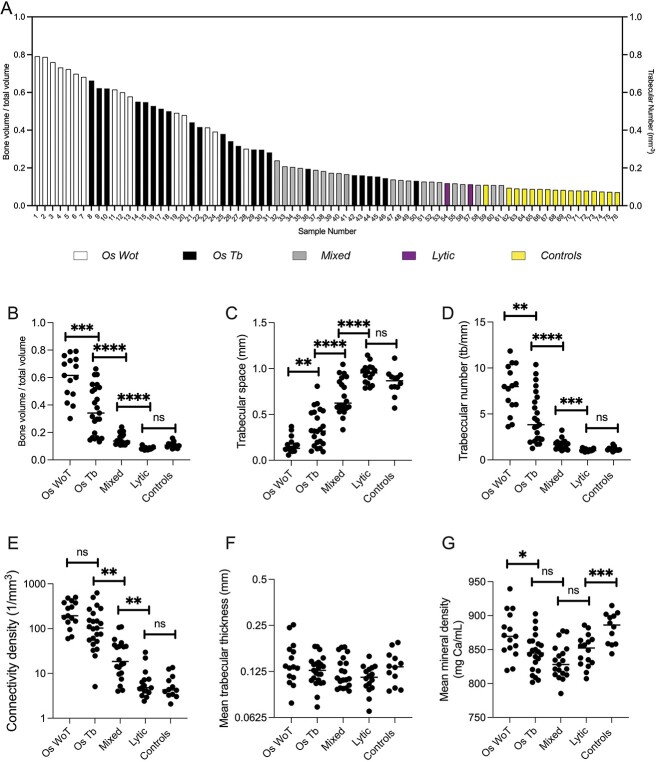
骨转移是前列腺癌(PC)最严重、最普遍的后果,80% 以上的晚期 PC 患者都会出现骨转移。PCBM 会导致疼痛、病理性骨折和瘫痪。随着现代疗法提高了患者的生存率,越来越多的患者正在遭受这些灾难性后果的折磨。从影像学上看,PCBM 主要呈骨质硬化,但骨质异常形成的机制以及骨密度的病理性增加与骨折的关系尚不清楚。在本研究中,我们对一组 76 例尸体 PCBM 标本和 12 例无癌症标本作为对照进行了全面分析。我们使用微型计算机断层扫描来确定三维组织和量化骨骼特征,使用定量反向散射电子显微镜来描述矿物质含量和骨骼结构的细节,使用纳米压痕来确定机械性能,并对骨骼结构和组成进行组织学和免疫组化分析。我们定义了 4 种 PCBM 表型:溶骨型、混合溶解硬化型和 2 个骨硬化病变亚组--有残余骨小梁的和没有残余骨小梁的。骨硬化性病变的特点是在骨小梁表面和小梁间隙内有异常骨质堆积。这种异常骨的特点是裂隙密度较高、裂隙形态异常和裂隙方向不规则。然而,这种不规则骨与残留骨小梁之间的矿物质含量、硬度和微米级弹性模量没有区别。这种异常骨的胶原基质组织不规则,胶原 III 成分突出。这些特征表明,骨硬化性 PCBM 会像编织骨一样开始新的骨沉积;然而,这种病理基质缺乏后续的骨重塑、表面没有片状骨沉积以及胶原 III 的存在,使其有别于传统的编织骨。虽然矿化基质保留了正常的骨硬度和刚度特性,但由于缺乏纤维各向异性,骨小梁结构受到损害,这可能会对临床产生影响。
Sclerotic prostate cancer bone metastasis: woven bone lesions with a twist.
Bone metastases are the most severe and prevalent consequences of prostate cancer (PC), affecting more than 80% of patients with advanced PC. PCBMs generate pain, pathological fractures, and paralysis. As modern therapies increase survival, more patients are suffering from these catastrophic consequences. Radiographically, PCBMs are predominantly osteosclerotic, but the mechanisms of abnormal bone formation and how this pathological increase in bone density is related to fractures are unclear. In this study, we conducted a comprehensive analysis on a cohort of 76 cadaveric PCBM specimens and 12 cancer-free specimens as controls. We used micro-computed tomography to determine 3D organization and quantify bone characteristics, quantitative backscattering electron microscopy to characterize mineral content and details in bone structure, nanoindentation to determine mechanical properties, and histological and immunohistochemical analysis of bone structure and composition. We define 4 PCBM phenotypes: osteolytic, mixed lytic-sclerotic, and 2 subgroups of osteosclerotic lesions-those with residual trabeculae, and others without residual trabeculae. The osteosclerotic lesions are characterized by the presence of abnormal bone accumulated on trabeculae surfaces and within intertrabecular spaces. This abnormal bone is characterized by higher lacunae density, abnormal lacunae morphology, and irregular lacunae orientation. However, mineral content, hardness, and elastic modulus at micron-scale were indistinguishable between this irregular bone and residual trabeculae. The collagen matrix of this abnormal bone presents with irregular organization and a prominent collagen III composition. These characteristics suggest that osteosclerotic PCBMs initiate new bone deposition as woven bone; however, the lack of subsequent bone remodeling, absence of lamellar bone deposition on its surface, and presence of collagen III distinguish this pathologic matrix from conventional woven bone. Although the mineralized matrix retains normal bone hardness and stiffness properties, the lack of fibril anisotropy presents a compromised trabecular structure, which may have clinical implications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


