Annerixt Gribnau, Gert J. Geurtsen, Hanna C. Willems, Jeroen Hermanides, Mark L. van Zuylen
{"title":"调整后的蒙特利尔认知评估与神经心理学评估在诊断术后神经认知障碍方面的比较。","authors":"Annerixt Gribnau, Gert J. Geurtsen, Hanna C. Willems, Jeroen Hermanides, Mark L. van Zuylen","doi":"10.1111/anae.16424","DOIUrl":null,"url":null,"abstract":"<p>The current gold standard neuropsychological assessment for detecting postoperative neurocognitive disorders is too time-consuming, costly and burdensome to use in clinical practice. Brief screening instruments, such as the Montreal Cognitive Assessment (MoCA), are used frequently instead. However, previous research by our team suggested that the original MoCA is not suitable to detect postoperative neurocognitive disorders in older adult surgical patients [<span>1</span>]. To improve the accuracy of the MoCA, Kessels et al. presented norms controlling for age, sex and educational level [<span>2</span>]. Accordingly, our study aimed to compare the performance of the adjusted MoCA score in diagnosing postoperative neurocognitive disorder.</p><p>We prospectively enrolled patients aged ≥ 65 y scheduled for elective surgery, involving any type of anaesthesia or surgical procedure, from September 2019 to January 2021, after approval by our local research ethics committee. Patients who were not fluent in Dutch, had pre-operative cognitive impairment, severe hearing impairment or needed several procedures under anaesthesia were not studied. The original study is described in full elsewhere [<span>1</span>]. Simultaneous administration of neuropsychological assessment and MoCA occurred pre-operatively and 30–60 days postoperatively, using alternate versions to minimise practice effect. Performance on neuropsychological assessment was reported as T-scores after comparison to a Dutch norm group (https://andi.nl). For neuropsychological assessment, a decline of 1–2 SD on ≥ 1 cognitive domain score indicated mild postoperative cognitive disorder, and ≥ 2 SD decline indicated major postoperative neurocognitive disorder [<span>3</span>]. In the post hoc analysis, we transformed the original, education-uncorrected, MoCA scores to percentiles according to Kessels et al. [<span>2</span>]. Mild postoperative neurocognitive disorder was defined as a reliable change index decrease of 1–2 SD [<span>4</span>] and ≥ 2 SD decline indicated major postoperative neurocognitive disorder. Test–retest reliability was measured by intraclass correlation coefficient. Data were missing completely at random and were imputed.</p><p>Sensitivity, specificity and area under the receiver operating characteristic curve of the adjusted MoCA were calculated. We examined pre-operative, postoperative and pre- to postoperative correlations of MoCA and total neuropsychological assessment and domain scores. We transformed the outcome to z-scores to assess agreement between MoCA and neuropsychological assessment by Bland–Altman plots. Ordinary or regression limits of agreement were chosen based on the presence or absence of proportional bias [<span>5</span>].</p><p>A total of 73 patients completed neuropsychological assessment and MoCA. Baseline characteristics are detailed in online Supporting Information Appendix S1. Neuropsychological assessment identified 14 (19%) cases of postoperative neurocognitive disorder and MoCA diagnosed 15 (21%) patients with cognitive disorders. Only two cases were diagnosed by both instruments (Table 1). Neuropsychological assessment classified all patients with mild postoperative neurocognitive disorder and MoCA diagnosed three patients with major cognitive disorder; however, only one of these cases was also diagnosed with postoperative neurocognitive disorder by neuropsychological assessment. Test–retest reliability of the adjusted MoCA was moderate (online Supporting Information Appendix S2).</p><p>Sensitivity and specificity of the adjusted MoCA were 0.14 (95%CI 0.03–0.38) and 0.78 (95%CI 0.66–0.87), respectively. The area under the receiver operating characteristic curve was 0.54 (95%CI 0.38–0.70). The correlations between pre-operative adjusted MoCA and neuropsychological assessment domain scores were weak to moderate (r = 0.12–0.48). Postoperative correlations were very weak to weak (r = -0.03–0.28) and pre- to postoperative MoCA correlations very weak (r = -0.10–0.09) (online Supporting Information Appendix S3). There was little agreement between pre-operative and postoperative MoCA scores compared with total neuropsychological assessment scores as well as domain scores (Fig. 1, online Supporting Information Appendices S4 and S5).</p><p>Our results suggest that the MoCA, despite adjustments for age, sex and educational level, is inadequate for diagnosing postoperative neurocognitive disorders in older adult elective surgical patients. It should not be used for clinical or research purposes for postoperative neurocognitive disorders, aligning with our previous research [<span>1</span>]. Sensitivity and specificity were comparable between adjusted (0.14–0.78) and original MoCA (0.21–0.84), respectively. Possible inadequacy of the MoCA could arise because of the subtlety in cognitive change in patients with postoperative neurocognitive disorders, as MoCA is only tailored for monitoring large cognitive changes in patients with dementia [<span>6</span>]. Additionally, studies showed a limited correlation between MoCA items and corresponding neuropsychological assessment scores, questioning the validity of the MoCA items and their comparability with neuropsychological assessment [<span>7</span>].</p><p>A limitation is the lack of a uniform definition for postoperative neurocognitive dysfunction. We chose the recommended approach using cognitive domain scores, but a different definition could possibly alter the results [<span>3</span>]. However, we compared the two diagnosing tools without the need for a definition by measuring agreement and correlations. Furthermore, various tests are used across studies for the gold standard neuropsychological assessment [<span>8</span>]. A strength was that MoCA was administered by trained staff.</p><p>We hypothesise that these findings extend to other brief cognitive tests, like the Mini-Mental State Exam, and, therefore, recommend caution in their use for diagnosing postoperative neurocognitive disorders. Collectively, our findings underscore the need for an adequate brief diagnostic tool tailored for postoperative neurocognitive disorder as existing brief instruments, such as the (adjusted) MoCA, seem inadequate.</p>","PeriodicalId":7742,"journal":{"name":"Anaesthesia","volume":"79 11","pages":"1250-1252"},"PeriodicalIF":6.9000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16424","citationCount":"0","resultStr":"{\"title\":\"Comparison between adjusted Montreal Cognitive Assessment and neuropsychological assessment for diagnosing postoperative neurocognitive disorders\",\"authors\":\"Annerixt Gribnau, Gert J. Geurtsen, Hanna C. Willems, Jeroen Hermanides, Mark L. van Zuylen\",\"doi\":\"10.1111/anae.16424\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The current gold standard neuropsychological assessment for detecting postoperative neurocognitive disorders is too time-consuming, costly and burdensome to use in clinical practice. Brief screening instruments, such as the Montreal Cognitive Assessment (MoCA), are used frequently instead. However, previous research by our team suggested that the original MoCA is not suitable to detect postoperative neurocognitive disorders in older adult surgical patients [<span>1</span>]. To improve the accuracy of the MoCA, Kessels et al. presented norms controlling for age, sex and educational level [<span>2</span>]. Accordingly, our study aimed to compare the performance of the adjusted MoCA score in diagnosing postoperative neurocognitive disorder.</p><p>We prospectively enrolled patients aged ≥ 65 y scheduled for elective surgery, involving any type of anaesthesia or surgical procedure, from September 2019 to January 2021, after approval by our local research ethics committee. Patients who were not fluent in Dutch, had pre-operative cognitive impairment, severe hearing impairment or needed several procedures under anaesthesia were not studied. The original study is described in full elsewhere [<span>1</span>]. Simultaneous administration of neuropsychological assessment and MoCA occurred pre-operatively and 30–60 days postoperatively, using alternate versions to minimise practice effect. Performance on neuropsychological assessment was reported as T-scores after comparison to a Dutch norm group (https://andi.nl). For neuropsychological assessment, a decline of 1–2 SD on ≥ 1 cognitive domain score indicated mild postoperative cognitive disorder, and ≥ 2 SD decline indicated major postoperative neurocognitive disorder [<span>3</span>]. In the post hoc analysis, we transformed the original, education-uncorrected, MoCA scores to percentiles according to Kessels et al. [<span>2</span>]. Mild postoperative neurocognitive disorder was defined as a reliable change index decrease of 1–2 SD [<span>4</span>] and ≥ 2 SD decline indicated major postoperative neurocognitive disorder. Test–retest reliability was measured by intraclass correlation coefficient. Data were missing completely at random and were imputed.</p><p>Sensitivity, specificity and area under the receiver operating characteristic curve of the adjusted MoCA were calculated. We examined pre-operative, postoperative and pre- to postoperative correlations of MoCA and total neuropsychological assessment and domain scores. We transformed the outcome to z-scores to assess agreement between MoCA and neuropsychological assessment by Bland–Altman plots. Ordinary or regression limits of agreement were chosen based on the presence or absence of proportional bias [<span>5</span>].</p><p>A total of 73 patients completed neuropsychological assessment and MoCA. Baseline characteristics are detailed in online Supporting Information Appendix S1. Neuropsychological assessment identified 14 (19%) cases of postoperative neurocognitive disorder and MoCA diagnosed 15 (21%) patients with cognitive disorders. Only two cases were diagnosed by both instruments (Table 1). Neuropsychological assessment classified all patients with mild postoperative neurocognitive disorder and MoCA diagnosed three patients with major cognitive disorder; however, only one of these cases was also diagnosed with postoperative neurocognitive disorder by neuropsychological assessment. Test–retest reliability of the adjusted MoCA was moderate (online Supporting Information Appendix S2).</p><p>Sensitivity and specificity of the adjusted MoCA were 0.14 (95%CI 0.03–0.38) and 0.78 (95%CI 0.66–0.87), respectively. The area under the receiver operating characteristic curve was 0.54 (95%CI 0.38–0.70). The correlations between pre-operative adjusted MoCA and neuropsychological assessment domain scores were weak to moderate (r = 0.12–0.48). Postoperative correlations were very weak to weak (r = -0.03–0.28) and pre- to postoperative MoCA correlations very weak (r = -0.10–0.09) (online Supporting Information Appendix S3). There was little agreement between pre-operative and postoperative MoCA scores compared with total neuropsychological assessment scores as well as domain scores (Fig. 1, online Supporting Information Appendices S4 and S5).</p><p>Our results suggest that the MoCA, despite adjustments for age, sex and educational level, is inadequate for diagnosing postoperative neurocognitive disorders in older adult elective surgical patients. It should not be used for clinical or research purposes for postoperative neurocognitive disorders, aligning with our previous research [<span>1</span>]. Sensitivity and specificity were comparable between adjusted (0.14–0.78) and original MoCA (0.21–0.84), respectively. Possible inadequacy of the MoCA could arise because of the subtlety in cognitive change in patients with postoperative neurocognitive disorders, as MoCA is only tailored for monitoring large cognitive changes in patients with dementia [<span>6</span>]. Additionally, studies showed a limited correlation between MoCA items and corresponding neuropsychological assessment scores, questioning the validity of the MoCA items and their comparability with neuropsychological assessment [<span>7</span>].</p><p>A limitation is the lack of a uniform definition for postoperative neurocognitive dysfunction. We chose the recommended approach using cognitive domain scores, but a different definition could possibly alter the results [<span>3</span>]. However, we compared the two diagnosing tools without the need for a definition by measuring agreement and correlations. Furthermore, various tests are used across studies for the gold standard neuropsychological assessment [<span>8</span>]. A strength was that MoCA was administered by trained staff.</p><p>We hypothesise that these findings extend to other brief cognitive tests, like the Mini-Mental State Exam, and, therefore, recommend caution in their use for diagnosing postoperative neurocognitive disorders. Collectively, our findings underscore the need for an adequate brief diagnostic tool tailored for postoperative neurocognitive disorder as existing brief instruments, such as the (adjusted) MoCA, seem inadequate.</p>\",\"PeriodicalId\":7742,\"journal\":{\"name\":\"Anaesthesia\",\"volume\":\"79 11\",\"pages\":\"1250-1252\"},\"PeriodicalIF\":6.9000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16424\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anaesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.16424\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia","FirstCategoryId":"3","ListUrlMain":"https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.16424","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Comparison between adjusted Montreal Cognitive Assessment and neuropsychological assessment for diagnosing postoperative neurocognitive disorders
The current gold standard neuropsychological assessment for detecting postoperative neurocognitive disorders is too time-consuming, costly and burdensome to use in clinical practice. Brief screening instruments, such as the Montreal Cognitive Assessment (MoCA), are used frequently instead. However, previous research by our team suggested that the original MoCA is not suitable to detect postoperative neurocognitive disorders in older adult surgical patients [1]. To improve the accuracy of the MoCA, Kessels et al. presented norms controlling for age, sex and educational level [2]. Accordingly, our study aimed to compare the performance of the adjusted MoCA score in diagnosing postoperative neurocognitive disorder.
We prospectively enrolled patients aged ≥ 65 y scheduled for elective surgery, involving any type of anaesthesia or surgical procedure, from September 2019 to January 2021, after approval by our local research ethics committee. Patients who were not fluent in Dutch, had pre-operative cognitive impairment, severe hearing impairment or needed several procedures under anaesthesia were not studied. The original study is described in full elsewhere [1]. Simultaneous administration of neuropsychological assessment and MoCA occurred pre-operatively and 30–60 days postoperatively, using alternate versions to minimise practice effect. Performance on neuropsychological assessment was reported as T-scores after comparison to a Dutch norm group (https://andi.nl). For neuropsychological assessment, a decline of 1–2 SD on ≥ 1 cognitive domain score indicated mild postoperative cognitive disorder, and ≥ 2 SD decline indicated major postoperative neurocognitive disorder [3]. In the post hoc analysis, we transformed the original, education-uncorrected, MoCA scores to percentiles according to Kessels et al. [2]. Mild postoperative neurocognitive disorder was defined as a reliable change index decrease of 1–2 SD [4] and ≥ 2 SD decline indicated major postoperative neurocognitive disorder. Test–retest reliability was measured by intraclass correlation coefficient. Data were missing completely at random and were imputed.
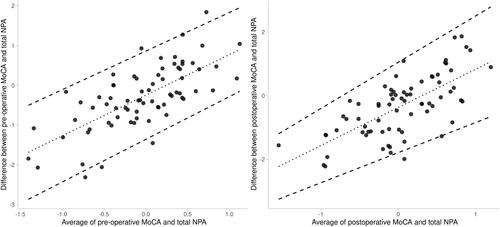
Sensitivity, specificity and area under the receiver operating characteristic curve of the adjusted MoCA were calculated. We examined pre-operative, postoperative and pre- to postoperative correlations of MoCA and total neuropsychological assessment and domain scores. We transformed the outcome to z-scores to assess agreement between MoCA and neuropsychological assessment by Bland–Altman plots. Ordinary or regression limits of agreement were chosen based on the presence or absence of proportional bias [5].
A total of 73 patients completed neuropsychological assessment and MoCA. Baseline characteristics are detailed in online Supporting Information Appendix S1. Neuropsychological assessment identified 14 (19%) cases of postoperative neurocognitive disorder and MoCA diagnosed 15 (21%) patients with cognitive disorders. Only two cases were diagnosed by both instruments (Table 1). Neuropsychological assessment classified all patients with mild postoperative neurocognitive disorder and MoCA diagnosed three patients with major cognitive disorder; however, only one of these cases was also diagnosed with postoperative neurocognitive disorder by neuropsychological assessment. Test–retest reliability of the adjusted MoCA was moderate (online Supporting Information Appendix S2).
Sensitivity and specificity of the adjusted MoCA were 0.14 (95%CI 0.03–0.38) and 0.78 (95%CI 0.66–0.87), respectively. The area under the receiver operating characteristic curve was 0.54 (95%CI 0.38–0.70). The correlations between pre-operative adjusted MoCA and neuropsychological assessment domain scores were weak to moderate (r = 0.12–0.48). Postoperative correlations were very weak to weak (r = -0.03–0.28) and pre- to postoperative MoCA correlations very weak (r = -0.10–0.09) (online Supporting Information Appendix S3). There was little agreement between pre-operative and postoperative MoCA scores compared with total neuropsychological assessment scores as well as domain scores (Fig. 1, online Supporting Information Appendices S4 and S5).
Our results suggest that the MoCA, despite adjustments for age, sex and educational level, is inadequate for diagnosing postoperative neurocognitive disorders in older adult elective surgical patients. It should not be used for clinical or research purposes for postoperative neurocognitive disorders, aligning with our previous research [1]. Sensitivity and specificity were comparable between adjusted (0.14–0.78) and original MoCA (0.21–0.84), respectively. Possible inadequacy of the MoCA could arise because of the subtlety in cognitive change in patients with postoperative neurocognitive disorders, as MoCA is only tailored for monitoring large cognitive changes in patients with dementia [6]. Additionally, studies showed a limited correlation between MoCA items and corresponding neuropsychological assessment scores, questioning the validity of the MoCA items and their comparability with neuropsychological assessment [7].
A limitation is the lack of a uniform definition for postoperative neurocognitive dysfunction. We chose the recommended approach using cognitive domain scores, but a different definition could possibly alter the results [3]. However, we compared the two diagnosing tools without the need for a definition by measuring agreement and correlations. Furthermore, various tests are used across studies for the gold standard neuropsychological assessment [8]. A strength was that MoCA was administered by trained staff.
We hypothesise that these findings extend to other brief cognitive tests, like the Mini-Mental State Exam, and, therefore, recommend caution in their use for diagnosing postoperative neurocognitive disorders. Collectively, our findings underscore the need for an adequate brief diagnostic tool tailored for postoperative neurocognitive disorder as existing brief instruments, such as the (adjusted) MoCA, seem inadequate.
期刊介绍:
The official journal of the Association of Anaesthetists is Anaesthesia. It is a comprehensive international publication that covers a wide range of topics. The journal focuses on general and regional anaesthesia, as well as intensive care and pain therapy. It includes original articles that have undergone peer review, covering all aspects of these fields, including research on equipment.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


