{"title":"耐甲氧西林金黄色葡萄球菌菌血症患者万古霉素浓度-时间曲线/最低抑制浓度的前 24 小时面积对治疗结果的影响。","authors":"Mika Higashi, Takafumi Nakano, Keisuke Sato, Yukiomi Eguchi, Norihiro Moriwaki, Mitsuhiro Kamada, Tadahiro Ikeuchi, Susumu Kaneshige, Masanobu Uchiyama, Toshinobu Hayashi, Atsushi Togawa, Koichi Matsuo, Hidetoshi Kamimura","doi":"10.14740/jocmr5238","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vancomycin regimens are designed to achieve an area under the concentration-time curve/minimum inhibitory concentration (AUC/MIC) ratio ranging between 400 and 600 µg·h/mL in the steady state. However, in cases of critical infections such as bacteremia requiring an early treatment approach, the clinical course may be affected by the AUC/MIC before reaching the steady state, that is, the AUC/MIC values 24 h after the first dose (first 24-h AUC/MIC). This study evaluated the relationship between the first 24-h AUC/MIC and the clinical course of methicillin-resistant <i>Staphylococcus aureus</i> (MRSA) infection.</p><p><strong>Methods: </strong>We retrospectively reviewed the records of patients with MRSA bacteremia in a university hospital between 2015 and 2022. The first 24-h AUC/MIC cutoff was set at 300 µg·h/mL based on the results of early response, and eligible patients were divided into groups with a first 24-h AUC/MIC either < 300 µg·h/mL (< 300 group, n = 32) or ≥ 300 µg·h/mL (≥ 300 group, n = 38). The primary endpoint was the rate of treatment efficacy, and the secondary endpoints were time to clinical and bacteriological improvement and 30-day survival rate.</p><p><strong>Results: </strong>Treatment efficacy and 30-day survival rates were not significantly different between the two groups (78.1% vs. 79.0%, P = 0.933 and 83.9% vs. 87.2%, P = 0.674, respectively). Among patients who showed treatment efficacy, the median time to clinical and bacteriological improvement was 11.5 days and 8.0 days in the < 300 and ≥ 300 groups, respectively; compared to the ≥ 300 group, the < 300 group had a significantly longer time to improvement (P = 0.001).</p><p><strong>Conclusions: </strong>The first 24-h AUC/MIC had no effect on the treatment efficacy and 30-day survival rates. However, the time to clinical and bacteriological improvement was significantly prolonged in the < 300 group, indicating that the first 24-h AUC/MIC does not affect the rate of therapeutic efficacy but may affect the treatment period.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 7-8","pages":"325-334"},"PeriodicalIF":2.0000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11349129/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of the First Twenty-Four-Hour Area Under the Concentration-Time Curve/Minimum Inhibitory Concentration of Vancomycin on Treatment Outcomes in Patients With Methicillin-Resistant <i>Staphylococcus aureus</i> Bacteremia.\",\"authors\":\"Mika Higashi, Takafumi Nakano, Keisuke Sato, Yukiomi Eguchi, Norihiro Moriwaki, Mitsuhiro Kamada, Tadahiro Ikeuchi, Susumu Kaneshige, Masanobu Uchiyama, Toshinobu Hayashi, Atsushi Togawa, Koichi Matsuo, Hidetoshi Kamimura\",\"doi\":\"10.14740/jocmr5238\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Vancomycin regimens are designed to achieve an area under the concentration-time curve/minimum inhibitory concentration (AUC/MIC) ratio ranging between 400 and 600 µg·h/mL in the steady state. However, in cases of critical infections such as bacteremia requiring an early treatment approach, the clinical course may be affected by the AUC/MIC before reaching the steady state, that is, the AUC/MIC values 24 h after the first dose (first 24-h AUC/MIC). This study evaluated the relationship between the first 24-h AUC/MIC and the clinical course of methicillin-resistant <i>Staphylococcus aureus</i> (MRSA) infection.</p><p><strong>Methods: </strong>We retrospectively reviewed the records of patients with MRSA bacteremia in a university hospital between 2015 and 2022. The first 24-h AUC/MIC cutoff was set at 300 µg·h/mL based on the results of early response, and eligible patients were divided into groups with a first 24-h AUC/MIC either < 300 µg·h/mL (< 300 group, n = 32) or ≥ 300 µg·h/mL (≥ 300 group, n = 38). The primary endpoint was the rate of treatment efficacy, and the secondary endpoints were time to clinical and bacteriological improvement and 30-day survival rate.</p><p><strong>Results: </strong>Treatment efficacy and 30-day survival rates were not significantly different between the two groups (78.1% vs. 79.0%, P = 0.933 and 83.9% vs. 87.2%, P = 0.674, respectively). Among patients who showed treatment efficacy, the median time to clinical and bacteriological improvement was 11.5 days and 8.0 days in the < 300 and ≥ 300 groups, respectively; compared to the ≥ 300 group, the < 300 group had a significantly longer time to improvement (P = 0.001).</p><p><strong>Conclusions: </strong>The first 24-h AUC/MIC had no effect on the treatment efficacy and 30-day survival rates. However, the time to clinical and bacteriological improvement was significantly prolonged in the < 300 group, indicating that the first 24-h AUC/MIC does not affect the rate of therapeutic efficacy but may affect the treatment period.</p>\",\"PeriodicalId\":94329,\"journal\":{\"name\":\"Journal of clinical medicine research\",\"volume\":\"16 7-8\",\"pages\":\"325-334\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11349129/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of clinical medicine research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jocmr5238\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr5238","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Impact of the First Twenty-Four-Hour Area Under the Concentration-Time Curve/Minimum Inhibitory Concentration of Vancomycin on Treatment Outcomes in Patients With Methicillin-Resistant Staphylococcus aureus Bacteremia.
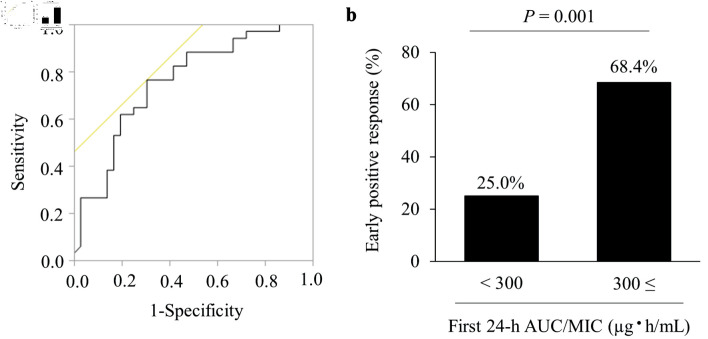
Background: Vancomycin regimens are designed to achieve an area under the concentration-time curve/minimum inhibitory concentration (AUC/MIC) ratio ranging between 400 and 600 µg·h/mL in the steady state. However, in cases of critical infections such as bacteremia requiring an early treatment approach, the clinical course may be affected by the AUC/MIC before reaching the steady state, that is, the AUC/MIC values 24 h after the first dose (first 24-h AUC/MIC). This study evaluated the relationship between the first 24-h AUC/MIC and the clinical course of methicillin-resistant Staphylococcus aureus (MRSA) infection.
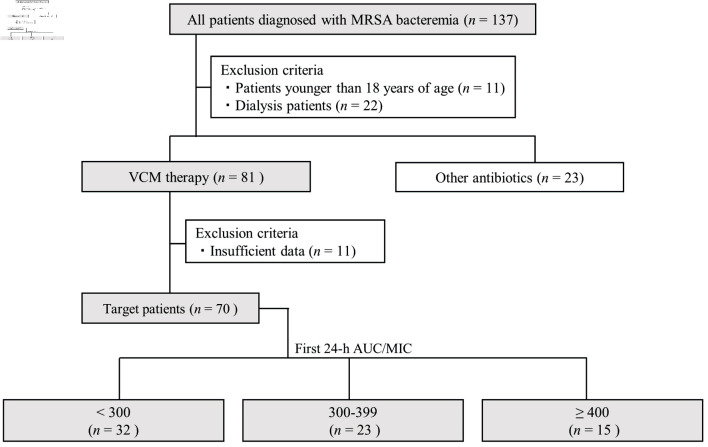
Methods: We retrospectively reviewed the records of patients with MRSA bacteremia in a university hospital between 2015 and 2022. The first 24-h AUC/MIC cutoff was set at 300 µg·h/mL based on the results of early response, and eligible patients were divided into groups with a first 24-h AUC/MIC either < 300 µg·h/mL (< 300 group, n = 32) or ≥ 300 µg·h/mL (≥ 300 group, n = 38). The primary endpoint was the rate of treatment efficacy, and the secondary endpoints were time to clinical and bacteriological improvement and 30-day survival rate.
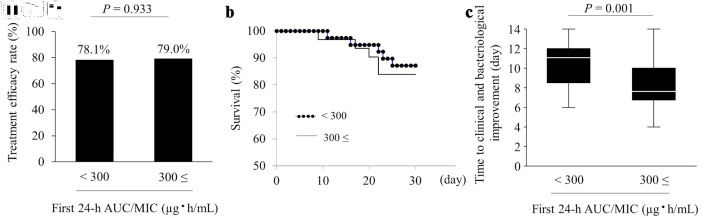
Results: Treatment efficacy and 30-day survival rates were not significantly different between the two groups (78.1% vs. 79.0%, P = 0.933 and 83.9% vs. 87.2%, P = 0.674, respectively). Among patients who showed treatment efficacy, the median time to clinical and bacteriological improvement was 11.5 days and 8.0 days in the < 300 and ≥ 300 groups, respectively; compared to the ≥ 300 group, the < 300 group had a significantly longer time to improvement (P = 0.001).
Conclusions: The first 24-h AUC/MIC had no effect on the treatment efficacy and 30-day survival rates. However, the time to clinical and bacteriological improvement was significantly prolonged in the < 300 group, indicating that the first 24-h AUC/MIC does not affect the rate of therapeutic efficacy but may affect the treatment period.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


