Annelies E de Weerd, Dave L Roelen, Michiel G H Betjes, Marian C Clahsen-van Groningen, Geert W Haasnoot, Marcia M L Kho, Marlies E J Reinders, Joke I Roodnat, David Severs, Gonca E Karahan, Jacqueline van de Wetering
{"title":"在交叉配型阳性的活体供肾移植中,抗HLA II类抗体最难脱敏:患者系列。","authors":"Annelies E de Weerd, Dave L Roelen, Michiel G H Betjes, Marian C Clahsen-van Groningen, Geert W Haasnoot, Marcia M L Kho, Marlies E J Reinders, Joke I Roodnat, David Severs, Gonca E Karahan, Jacqueline van de Wetering","doi":"10.1097/TXD.0000000000001695","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In HLA-incompatible kidney transplantation, the efficacy of desensitization in terms of anti-HLA antibody kinetics is not well characterized. We present an overview of the course of anti-HLA antibodies throughout plasma exchange (PE) desensitization in a series of crossmatch-positive patients.</p><p><strong>Methods: </strong>All consecutive candidates in the Dutch HLA-incompatible kidney transplantation program between November 2012 and January 2022 were included. The eligibility criteria were a positive crossmatch with a living kidney donor and no options for compatible transplantation. Desensitization consisted of 5-10 PE with low-dose IVIg.</p><p><strong>Results: </strong>A total of 16 patient-donor pairs were included. Patients had median virtual panel-reactive antibody of 99.58%. Cumulative donor-specific anti-HLA antibody (cumDSA) mean fluorescence intensity (MFI) was 31 399 median, and immunodominant DSA (iDSA) MFI was 18 677 for class I and 21 893 for class II. Median anti-HLA antibody MFI response to desensitization was worse in class II as compared with class I (<i>P</i> < 0.001), particularly for HLA-DQ. Class I cumDSA MFI decreased 68% after 4 PE versus 53% in class II. The decrease between the fifth and the 10th PE sessions was modest with 21% in class I versus 9% in class II. Antibody-mediated rejection occurred in 85% of patients, with the iDSA directed to the same mismatched HLA as before desensitization, except for 3 patients, of whom 2 had vigorous rebound of antibodies to repeated mismatches (RMMs). Rebound was highest (86%) in RMM-DSA with prior grafts removed (transplantectomy n = 7), lower (39%) in non-RMM-DSA (n = 30), and lowest (11%) for RMM-DSA with in situ grafts (n = 5; <i>P</i> = 0.018 for RMM-DSA transplantectomy versus RMM-DSA graft in situ). With a median follow-up of 59 mo, 1 patient had died resulting in a death-censored graft survival of 73%.</p><p><strong>Conclusions: </strong>Patients with class II DSA, and particularly those directed against HLA-DQ locus, were difficult to desensitize.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 9","pages":"e1695"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11365629/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anti-HLA Class II Antibodies Are the Most Resistant to Desensitization in Crossmatch-positive Living-donor Kidney Transplantations: A Patient Series.\",\"authors\":\"Annelies E de Weerd, Dave L Roelen, Michiel G H Betjes, Marian C Clahsen-van Groningen, Geert W Haasnoot, Marcia M L Kho, Marlies E J Reinders, Joke I Roodnat, David Severs, Gonca E Karahan, Jacqueline van de Wetering\",\"doi\":\"10.1097/TXD.0000000000001695\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In HLA-incompatible kidney transplantation, the efficacy of desensitization in terms of anti-HLA antibody kinetics is not well characterized. We present an overview of the course of anti-HLA antibodies throughout plasma exchange (PE) desensitization in a series of crossmatch-positive patients.</p><p><strong>Methods: </strong>All consecutive candidates in the Dutch HLA-incompatible kidney transplantation program between November 2012 and January 2022 were included. The eligibility criteria were a positive crossmatch with a living kidney donor and no options for compatible transplantation. Desensitization consisted of 5-10 PE with low-dose IVIg.</p><p><strong>Results: </strong>A total of 16 patient-donor pairs were included. Patients had median virtual panel-reactive antibody of 99.58%. Cumulative donor-specific anti-HLA antibody (cumDSA) mean fluorescence intensity (MFI) was 31 399 median, and immunodominant DSA (iDSA) MFI was 18 677 for class I and 21 893 for class II. Median anti-HLA antibody MFI response to desensitization was worse in class II as compared with class I (<i>P</i> < 0.001), particularly for HLA-DQ. Class I cumDSA MFI decreased 68% after 4 PE versus 53% in class II. The decrease between the fifth and the 10th PE sessions was modest with 21% in class I versus 9% in class II. Antibody-mediated rejection occurred in 85% of patients, with the iDSA directed to the same mismatched HLA as before desensitization, except for 3 patients, of whom 2 had vigorous rebound of antibodies to repeated mismatches (RMMs). Rebound was highest (86%) in RMM-DSA with prior grafts removed (transplantectomy n = 7), lower (39%) in non-RMM-DSA (n = 30), and lowest (11%) for RMM-DSA with in situ grafts (n = 5; <i>P</i> = 0.018 for RMM-DSA transplantectomy versus RMM-DSA graft in situ). With a median follow-up of 59 mo, 1 patient had died resulting in a death-censored graft survival of 73%.</p><p><strong>Conclusions: </strong>Patients with class II DSA, and particularly those directed against HLA-DQ locus, were difficult to desensitize.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"10 9\",\"pages\":\"e1695\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11365629/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001695\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001695","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
Anti-HLA Class II Antibodies Are the Most Resistant to Desensitization in Crossmatch-positive Living-donor Kidney Transplantations: A Patient Series.
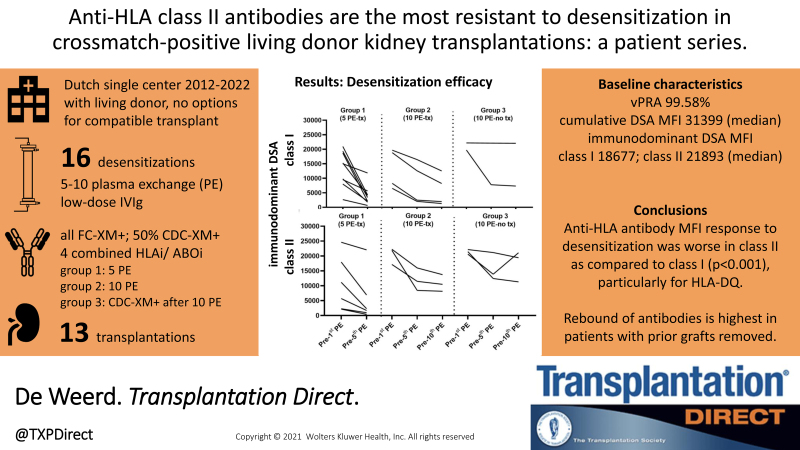
Background: In HLA-incompatible kidney transplantation, the efficacy of desensitization in terms of anti-HLA antibody kinetics is not well characterized. We present an overview of the course of anti-HLA antibodies throughout plasma exchange (PE) desensitization in a series of crossmatch-positive patients.
Methods: All consecutive candidates in the Dutch HLA-incompatible kidney transplantation program between November 2012 and January 2022 were included. The eligibility criteria were a positive crossmatch with a living kidney donor and no options for compatible transplantation. Desensitization consisted of 5-10 PE with low-dose IVIg.
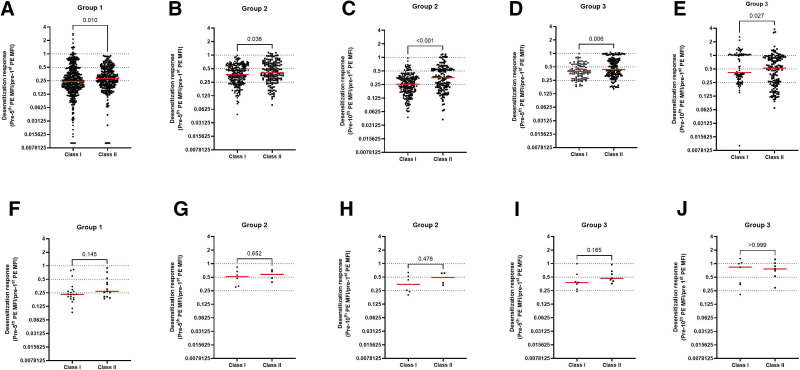
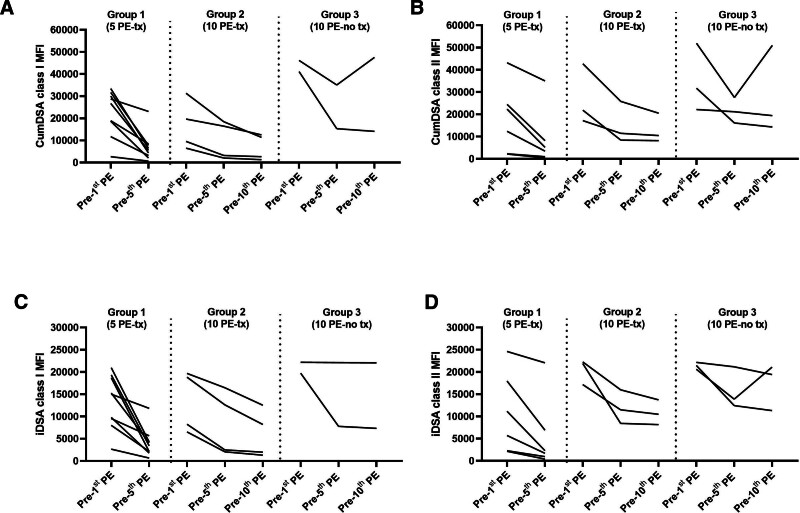
Results: A total of 16 patient-donor pairs were included. Patients had median virtual panel-reactive antibody of 99.58%. Cumulative donor-specific anti-HLA antibody (cumDSA) mean fluorescence intensity (MFI) was 31 399 median, and immunodominant DSA (iDSA) MFI was 18 677 for class I and 21 893 for class II. Median anti-HLA antibody MFI response to desensitization was worse in class II as compared with class I (P < 0.001), particularly for HLA-DQ. Class I cumDSA MFI decreased 68% after 4 PE versus 53% in class II. The decrease between the fifth and the 10th PE sessions was modest with 21% in class I versus 9% in class II. Antibody-mediated rejection occurred in 85% of patients, with the iDSA directed to the same mismatched HLA as before desensitization, except for 3 patients, of whom 2 had vigorous rebound of antibodies to repeated mismatches (RMMs). Rebound was highest (86%) in RMM-DSA with prior grafts removed (transplantectomy n = 7), lower (39%) in non-RMM-DSA (n = 30), and lowest (11%) for RMM-DSA with in situ grafts (n = 5; P = 0.018 for RMM-DSA transplantectomy versus RMM-DSA graft in situ). With a median follow-up of 59 mo, 1 patient had died resulting in a death-censored graft survival of 73%.
Conclusions: Patients with class II DSA, and particularly those directed against HLA-DQ locus, were difficult to desensitize.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


