Nicole Lefel, Hans van Suijlekom, Steven P C Cohen, Jan Willem Kallewaard, Jan Van Zundert
{"title":"11.颈源性头痛和枕神经痛。","authors":"Nicole Lefel, Hans van Suijlekom, Steven P C Cohen, Jan Willem Kallewaard, Jan Van Zundert","doi":"10.1111/papr.13405","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cervicogenic headache (CEH) and occipital neuralgia (ON) are headaches originating in the occiput and that radiate to the vertex. Because of the intimate relationship between structures based in the occiput and those in the upper cervical region, there is significant overlap between the presentation of CEH and ON. Diagnosis starts with a headache history to assess for diagnostic criteria formulated by the International Headache Society. Physical examination evaluates range of motion of the neck and the presence of tender areas or pressure points.</p><p><strong>Methods: </strong>The literature for the diagnosis and treatment of CEH and ON was searched from 2015 through August 2022, retrieved, and summarized.</p><p><strong>Results: </strong>Conservative treatment includes pain education and self-care, analgesic medication, physical therapy (such as reducing secondary muscle tension and improving posture), the use of TENS (transcutaneous electrical nerve stimulation), or a combination of the aforementioned treatments. Injection at various anatomical locations with local anesthetic with or without corticosteroids can provide pain relief for a short period. Deep cervical plexus block can result in improved pain for less than 6 months. In both CEH and ON, an occipital nerve block can provide important diagnostic information and improve pain in some patients, with PRF providing greater long-term pain control. Radiofrequency ablation of the cervical facet joints can result in improvement for over 1 year. Occipital nerve stimulation (ONS) should be considered for the treatment of refractory ON.</p><p><strong>Conclusion: </strong>The treatment of CEH preferentially consists of radiofrequency treatment of the facet joints, while for ON, pulsed radiofrequency of the occipital nerves is indicated. For refractory cases, ONS may be considered.</p>","PeriodicalId":19974,"journal":{"name":"Pain Practice","volume":" ","pages":"e13405"},"PeriodicalIF":2.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11680101/pdf/","citationCount":"0","resultStr":"{\"title\":\"11. Cervicogenic headache and occipital neuralgia.\",\"authors\":\"Nicole Lefel, Hans van Suijlekom, Steven P C Cohen, Jan Willem Kallewaard, Jan Van Zundert\",\"doi\":\"10.1111/papr.13405\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Cervicogenic headache (CEH) and occipital neuralgia (ON) are headaches originating in the occiput and that radiate to the vertex. Because of the intimate relationship between structures based in the occiput and those in the upper cervical region, there is significant overlap between the presentation of CEH and ON. Diagnosis starts with a headache history to assess for diagnostic criteria formulated by the International Headache Society. Physical examination evaluates range of motion of the neck and the presence of tender areas or pressure points.</p><p><strong>Methods: </strong>The literature for the diagnosis and treatment of CEH and ON was searched from 2015 through August 2022, retrieved, and summarized.</p><p><strong>Results: </strong>Conservative treatment includes pain education and self-care, analgesic medication, physical therapy (such as reducing secondary muscle tension and improving posture), the use of TENS (transcutaneous electrical nerve stimulation), or a combination of the aforementioned treatments. Injection at various anatomical locations with local anesthetic with or without corticosteroids can provide pain relief for a short period. Deep cervical plexus block can result in improved pain for less than 6 months. In both CEH and ON, an occipital nerve block can provide important diagnostic information and improve pain in some patients, with PRF providing greater long-term pain control. Radiofrequency ablation of the cervical facet joints can result in improvement for over 1 year. Occipital nerve stimulation (ONS) should be considered for the treatment of refractory ON.</p><p><strong>Conclusion: </strong>The treatment of CEH preferentially consists of radiofrequency treatment of the facet joints, while for ON, pulsed radiofrequency of the occipital nerves is indicated. For refractory cases, ONS may be considered.</p>\",\"PeriodicalId\":19974,\"journal\":{\"name\":\"Pain Practice\",\"volume\":\" \",\"pages\":\"e13405\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11680101/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pain Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/papr.13405\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/papr.13405","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
11. Cervicogenic headache and occipital neuralgia.
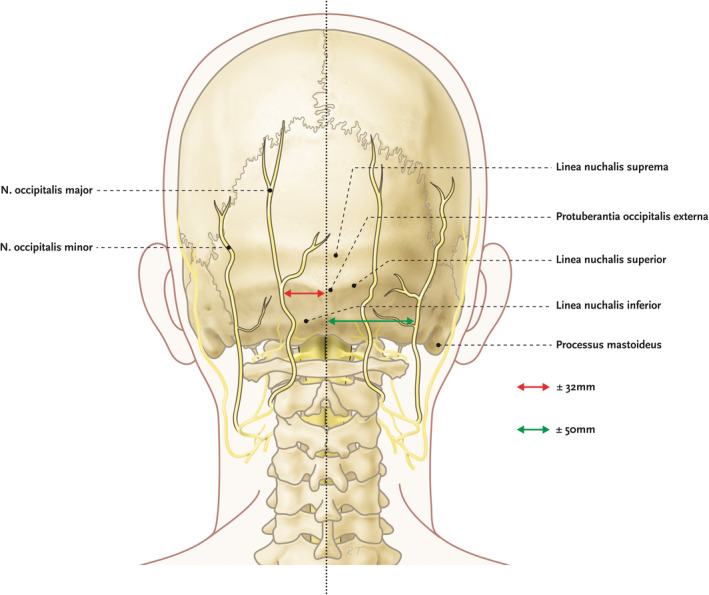
Introduction: Cervicogenic headache (CEH) and occipital neuralgia (ON) are headaches originating in the occiput and that radiate to the vertex. Because of the intimate relationship between structures based in the occiput and those in the upper cervical region, there is significant overlap between the presentation of CEH and ON. Diagnosis starts with a headache history to assess for diagnostic criteria formulated by the International Headache Society. Physical examination evaluates range of motion of the neck and the presence of tender areas or pressure points.
Methods: The literature for the diagnosis and treatment of CEH and ON was searched from 2015 through August 2022, retrieved, and summarized.
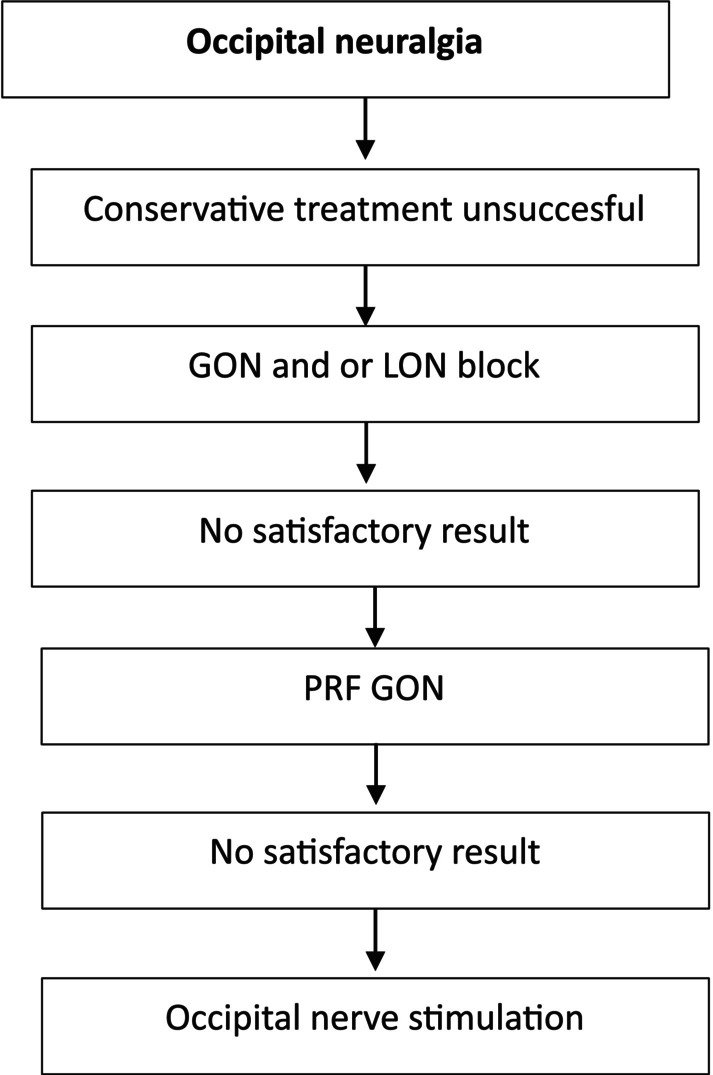
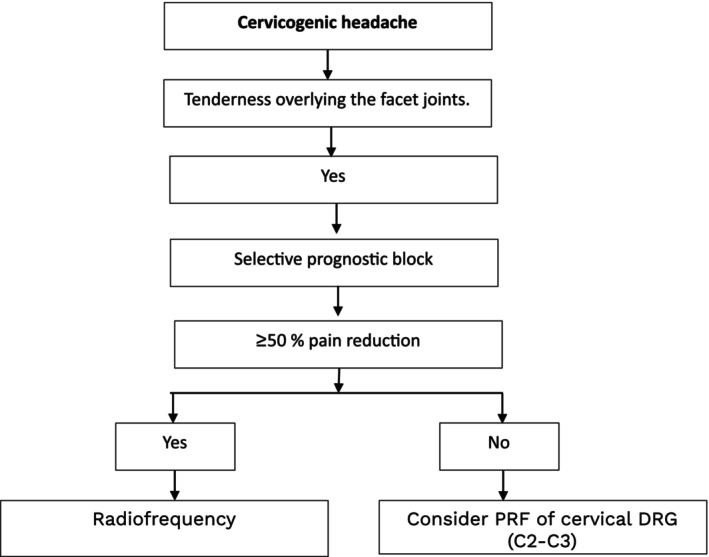
Results: Conservative treatment includes pain education and self-care, analgesic medication, physical therapy (such as reducing secondary muscle tension and improving posture), the use of TENS (transcutaneous electrical nerve stimulation), or a combination of the aforementioned treatments. Injection at various anatomical locations with local anesthetic with or without corticosteroids can provide pain relief for a short period. Deep cervical plexus block can result in improved pain for less than 6 months. In both CEH and ON, an occipital nerve block can provide important diagnostic information and improve pain in some patients, with PRF providing greater long-term pain control. Radiofrequency ablation of the cervical facet joints can result in improvement for over 1 year. Occipital nerve stimulation (ONS) should be considered for the treatment of refractory ON.
Conclusion: The treatment of CEH preferentially consists of radiofrequency treatment of the facet joints, while for ON, pulsed radiofrequency of the occipital nerves is indicated. For refractory cases, ONS may be considered.
期刊介绍:
Pain Practice, the official journal of the World Institute of Pain, publishes international multidisciplinary articles on pain and analgesia that provide its readership with up-to-date research, evaluation methods, and techniques for pain management. Special sections including the Consultant’s Corner, Images in Pain Practice, Case Studies from Mayo, Tutorials, and the Evidence-Based Medicine combine to give pain researchers, pain clinicians and pain fellows in training a systematic approach to continuing education in pain medicine. Prior to publication, all articles and reviews undergo peer review by at least two experts in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


