{"title":"比较损伤严重程度评分(ISS)和新损伤严重程度评分(NISS)对胸外伤患者的评估:回顾性队列研究。","authors":"He Jin, Yuanyuan Zhang, Qi Zhang, Lijuan Ouyang, Xueyao Li, Yiyan Zhang, Baosheng Yang, Junfeng Sun, Chaohui Wei, Guimei Yang, Li Guan, Shilan Luo, Junyu Zhu, Huaping Liang","doi":"10.1155/2024/4861308","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To explore the value of the injury severity score (ISS) and the new injury severity score (NISS) for evaluating injuries and predicting complications (pneumonia and respiratory failure) and poor prognoses (in-hospital tracheal intubation, extended length of hospital stay, ICU admission, prolonged ICU stay, and death) in patients with thoracic trauma.</p><p><strong>Methods: </strong>The data of consecutive patients with thoracic trauma who were admitted to the department of cardiothoracic surgery of a tertiary hospital between January 2018 and December 2021 were retrospectively collected. ISS and NISS were calculated for each patient. The study outcomes were complications and poor prognoses. The differences in ISS and NISS between patients with complications and poor prognoses and patients without the abovementioned conditions were compared using the Mann‒Whitney <i>U</i> test. Discrimination and calibration of ISS and NISS in predicting outcomes were compared using the area under the receiver operating characteristic (ROC) curve (AUC) and Hosmer‒Lemeshow (H-L) statistic.</p><p><strong>Results: </strong>A total of 310 patients were included. ISS and NISS of patients with complications and poor prognoses were greater than those of patients without complications and poor prognoses, respectively. The discrimination of ISS in predicting pneumonia, respiratory failure, in-hospital tracheal intubation, extended length of hospital stay, ICU admission, prolonged ICU stay, and death (AUCs: 0.609, 0.721, 0.848, 0.784, 0.763, 0.716, and 0.804, respectively) was not statistically significantly different from that of NISS in predicting the corresponding outcomes (AUCs: 0.628, 0.712, 0.795, 0.767, 0.750, 0.750, and 0.818, respectively). ISS showed better calibration than NISS for predicting pneumonia, respiratory failure, in-hospital tracheal intubation, extended length of hospital stay, and ICU admission but worse calibration for predicting prolonged ICU stay and death.</p><p><strong>Conclusion: </strong>ISS and NISS are both suitable for injury evaluation. There was no statistically significant difference in discrimination between ISS and NISS, but they had different calibrations when predicting different outcomes.</p>","PeriodicalId":11528,"journal":{"name":"Emergency Medicine International","volume":"2024 ","pages":"4861308"},"PeriodicalIF":0.8000,"publicationDate":"2024-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11364476/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of Injury Severity Score (ISS) and New Injury Severity Score (NISS) in the Evaluation of Thoracic Trauma Patients: A Retrospective Cohort Study.\",\"authors\":\"He Jin, Yuanyuan Zhang, Qi Zhang, Lijuan Ouyang, Xueyao Li, Yiyan Zhang, Baosheng Yang, Junfeng Sun, Chaohui Wei, Guimei Yang, Li Guan, Shilan Luo, Junyu Zhu, Huaping Liang\",\"doi\":\"10.1155/2024/4861308\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To explore the value of the injury severity score (ISS) and the new injury severity score (NISS) for evaluating injuries and predicting complications (pneumonia and respiratory failure) and poor prognoses (in-hospital tracheal intubation, extended length of hospital stay, ICU admission, prolonged ICU stay, and death) in patients with thoracic trauma.</p><p><strong>Methods: </strong>The data of consecutive patients with thoracic trauma who were admitted to the department of cardiothoracic surgery of a tertiary hospital between January 2018 and December 2021 were retrospectively collected. ISS and NISS were calculated for each patient. The study outcomes were complications and poor prognoses. The differences in ISS and NISS between patients with complications and poor prognoses and patients without the abovementioned conditions were compared using the Mann‒Whitney <i>U</i> test. Discrimination and calibration of ISS and NISS in predicting outcomes were compared using the area under the receiver operating characteristic (ROC) curve (AUC) and Hosmer‒Lemeshow (H-L) statistic.</p><p><strong>Results: </strong>A total of 310 patients were included. ISS and NISS of patients with complications and poor prognoses were greater than those of patients without complications and poor prognoses, respectively. The discrimination of ISS in predicting pneumonia, respiratory failure, in-hospital tracheal intubation, extended length of hospital stay, ICU admission, prolonged ICU stay, and death (AUCs: 0.609, 0.721, 0.848, 0.784, 0.763, 0.716, and 0.804, respectively) was not statistically significantly different from that of NISS in predicting the corresponding outcomes (AUCs: 0.628, 0.712, 0.795, 0.767, 0.750, 0.750, and 0.818, respectively). ISS showed better calibration than NISS for predicting pneumonia, respiratory failure, in-hospital tracheal intubation, extended length of hospital stay, and ICU admission but worse calibration for predicting prolonged ICU stay and death.</p><p><strong>Conclusion: </strong>ISS and NISS are both suitable for injury evaluation. There was no statistically significant difference in discrimination between ISS and NISS, but they had different calibrations when predicting different outcomes.</p>\",\"PeriodicalId\":11528,\"journal\":{\"name\":\"Emergency Medicine International\",\"volume\":\"2024 \",\"pages\":\"4861308\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2024-08-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11364476/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Emergency Medicine International\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/4861308\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Medicine International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2024/4861308","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
目的探讨损伤严重程度评分(ISS)和新损伤严重程度评分(NISS)对胸部创伤患者的损伤评估、并发症(肺炎和呼吸衰竭)和不良预后(院内气管插管、住院时间延长、入住ICU、ICU住院时间延长和死亡)预测的价值:回顾性收集2018年1月至2021年12月期间某三甲医院心胸外科连续收治的胸部创伤患者的数据。计算了每位患者的 ISS 和 NISS。研究结果为并发症和不良预后。采用 Mann-Whitney U 检验比较了有并发症和预后不良患者与无上述情况患者的 ISS 和 NISS 差异。使用接收者操作特征曲线(ROC)下面积(AUC)和Hosmer-Lemeshow(H-L)统计量比较了ISS和NISS在预测预后方面的区分度和校准度:共纳入 310 例患者。有并发症和预后不良患者的 ISS 和 NISS 分别高于无并发症和预后不良患者。ISS在预测肺炎、呼吸衰竭、院内气管插管、住院时间延长、ICU入院、ICU住院时间延长和死亡方面的区分度(AUC:0.609、0.721、0.848、0.784、0.763、0.716 和 0.804)在预测相应结果方面与 NISS(AUC 分别为 0.628、0.712、0.795、0.767、0.750、0.750 和 0.818)没有显著统计学差异。在预测肺炎、呼吸衰竭、院内气管插管、住院时间延长和入住重症监护室方面,ISS的校准效果优于NISS,但在预测重症监护室住院时间延长和死亡方面,ISS的校准效果较差:结论:ISS 和 NISS 都适用于损伤评估。结论:ISS 和 NISS 都适用于损伤评估,ISS 和 NISS 的区分度在统计学上没有明显差异,但它们在预测不同结果时有不同的定标。
Comparison of Injury Severity Score (ISS) and New Injury Severity Score (NISS) in the Evaluation of Thoracic Trauma Patients: A Retrospective Cohort Study.
Objective: To explore the value of the injury severity score (ISS) and the new injury severity score (NISS) for evaluating injuries and predicting complications (pneumonia and respiratory failure) and poor prognoses (in-hospital tracheal intubation, extended length of hospital stay, ICU admission, prolonged ICU stay, and death) in patients with thoracic trauma.
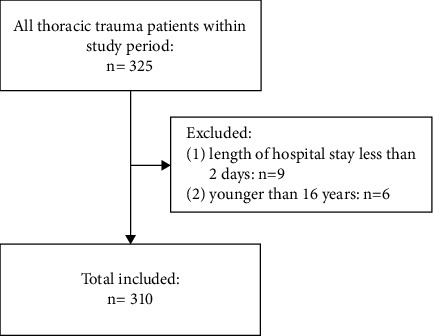
Methods: The data of consecutive patients with thoracic trauma who were admitted to the department of cardiothoracic surgery of a tertiary hospital between January 2018 and December 2021 were retrospectively collected. ISS and NISS were calculated for each patient. The study outcomes were complications and poor prognoses. The differences in ISS and NISS between patients with complications and poor prognoses and patients without the abovementioned conditions were compared using the Mann‒Whitney U test. Discrimination and calibration of ISS and NISS in predicting outcomes were compared using the area under the receiver operating characteristic (ROC) curve (AUC) and Hosmer‒Lemeshow (H-L) statistic.
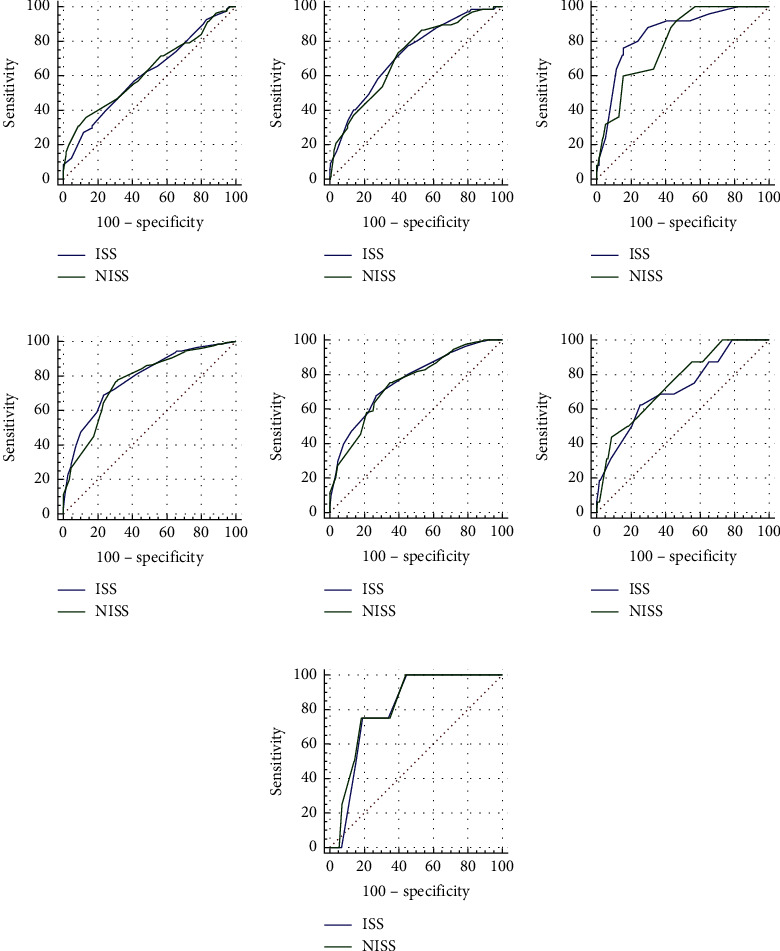
Results: A total of 310 patients were included. ISS and NISS of patients with complications and poor prognoses were greater than those of patients without complications and poor prognoses, respectively. The discrimination of ISS in predicting pneumonia, respiratory failure, in-hospital tracheal intubation, extended length of hospital stay, ICU admission, prolonged ICU stay, and death (AUCs: 0.609, 0.721, 0.848, 0.784, 0.763, 0.716, and 0.804, respectively) was not statistically significantly different from that of NISS in predicting the corresponding outcomes (AUCs: 0.628, 0.712, 0.795, 0.767, 0.750, 0.750, and 0.818, respectively). ISS showed better calibration than NISS for predicting pneumonia, respiratory failure, in-hospital tracheal intubation, extended length of hospital stay, and ICU admission but worse calibration for predicting prolonged ICU stay and death.
Conclusion: ISS and NISS are both suitable for injury evaluation. There was no statistically significant difference in discrimination between ISS and NISS, but they had different calibrations when predicting different outcomes.
期刊介绍:
Emergency Medicine International is a peer-reviewed, Open Access journal that provides a forum for doctors, nurses, paramedics and ambulance staff. The journal publishes original research articles, review articles, and clinical studies related to prehospital care, disaster preparedness and response, acute medical and paediatric emergencies, critical care, sports medicine, wound care, and toxicology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


