Mustafa Gerçek, Tomislav Skuljevic, Jochen Börgermann, Jan Gummert, Muhammed Gerçek
{"title":"冠状动脉旁路移植术中左心房阑尾截肢的围手术期效果。","authors":"Mustafa Gerçek, Tomislav Skuljevic, Jochen Börgermann, Jan Gummert, Muhammed Gerçek","doi":"10.1007/s00392-024-02529-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Left atrial appendage (LAA) amputation performed alongside cardiac surgery has become an increasingly established procedure to reduce stroke risk in patients with atrial fibrillation. As the recommendation levels for LAA amputation continue to rise, ample evidence assessing its perioperative safety and risk factors is of utmost interest.</p><p><strong>Methods: </strong>All patients who underwent isolated coronary artery bypass grafting (CABG) between 2018 and 2021 at two high-volume centers were retrospectively included in the study. Patients were divided into two groups-the CABG and CABG + LAA groups-based on whether they underwent concomitant LAA amputation. Propensity score matching (PS matching) was applied to ensure comparability between the groups. The primary endpoint was defined as a composite outcome comprising of all-cause mortality, stroke, and reoperation. Secondary endpoints included the components of the primary endpoint, perioperative outcome parameters, transfusion rates, and laboratory parameters.</p><p><strong>Results: </strong>A total of 3904 patients were included with 3038 and 866 in the CABG and CABG + LAA group, respectively. After PS matching each group consisted of 856 patients. The primary endpoint showed no significant differences between the CABG and CABG + LAA group (7.0% vs. 6.5% (OR 0.9 95% CI [0.64; 1.35], p = 0.70)). Similarly, there were no notable differences in the individual components of the composite endpoint: all-cause mortality (p = 0.84), stroke (p = 0.74), and reoperation (p = 0.50). Subgroup results did not show any relevant dissimilarity.</p><p><strong>Conclusion: </strong>The concomitant performance of LAA amputation is not associated with worse in-hospital outcomes, as measured by the composite endpoint of all-cause mortality, stroke, and reoperation.</p>","PeriodicalId":10474,"journal":{"name":"Clinical Research in Cardiology","volume":null,"pages":null},"PeriodicalIF":3.8000,"publicationDate":"2024-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Perioperative outcome of left atrial appendage amputation in coronary artery bypass grafting.\",\"authors\":\"Mustafa Gerçek, Tomislav Skuljevic, Jochen Börgermann, Jan Gummert, Muhammed Gerçek\",\"doi\":\"10.1007/s00392-024-02529-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Left atrial appendage (LAA) amputation performed alongside cardiac surgery has become an increasingly established procedure to reduce stroke risk in patients with atrial fibrillation. As the recommendation levels for LAA amputation continue to rise, ample evidence assessing its perioperative safety and risk factors is of utmost interest.</p><p><strong>Methods: </strong>All patients who underwent isolated coronary artery bypass grafting (CABG) between 2018 and 2021 at two high-volume centers were retrospectively included in the study. Patients were divided into two groups-the CABG and CABG + LAA groups-based on whether they underwent concomitant LAA amputation. Propensity score matching (PS matching) was applied to ensure comparability between the groups. The primary endpoint was defined as a composite outcome comprising of all-cause mortality, stroke, and reoperation. Secondary endpoints included the components of the primary endpoint, perioperative outcome parameters, transfusion rates, and laboratory parameters.</p><p><strong>Results: </strong>A total of 3904 patients were included with 3038 and 866 in the CABG and CABG + LAA group, respectively. After PS matching each group consisted of 856 patients. The primary endpoint showed no significant differences between the CABG and CABG + LAA group (7.0% vs. 6.5% (OR 0.9 95% CI [0.64; 1.35], p = 0.70)). Similarly, there were no notable differences in the individual components of the composite endpoint: all-cause mortality (p = 0.84), stroke (p = 0.74), and reoperation (p = 0.50). Subgroup results did not show any relevant dissimilarity.</p><p><strong>Conclusion: </strong>The concomitant performance of LAA amputation is not associated with worse in-hospital outcomes, as measured by the composite endpoint of all-cause mortality, stroke, and reoperation.</p>\",\"PeriodicalId\":10474,\"journal\":{\"name\":\"Clinical Research in Cardiology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2024-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Research in Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00392-024-02529-9\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Research in Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00392-024-02529-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
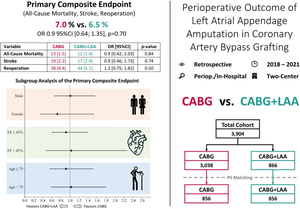
Perioperative outcome of left atrial appendage amputation in coronary artery bypass grafting.
Background: Left atrial appendage (LAA) amputation performed alongside cardiac surgery has become an increasingly established procedure to reduce stroke risk in patients with atrial fibrillation. As the recommendation levels for LAA amputation continue to rise, ample evidence assessing its perioperative safety and risk factors is of utmost interest.
Methods: All patients who underwent isolated coronary artery bypass grafting (CABG) between 2018 and 2021 at two high-volume centers were retrospectively included in the study. Patients were divided into two groups-the CABG and CABG + LAA groups-based on whether they underwent concomitant LAA amputation. Propensity score matching (PS matching) was applied to ensure comparability between the groups. The primary endpoint was defined as a composite outcome comprising of all-cause mortality, stroke, and reoperation. Secondary endpoints included the components of the primary endpoint, perioperative outcome parameters, transfusion rates, and laboratory parameters.
Results: A total of 3904 patients were included with 3038 and 866 in the CABG and CABG + LAA group, respectively. After PS matching each group consisted of 856 patients. The primary endpoint showed no significant differences between the CABG and CABG + LAA group (7.0% vs. 6.5% (OR 0.9 95% CI [0.64; 1.35], p = 0.70)). Similarly, there were no notable differences in the individual components of the composite endpoint: all-cause mortality (p = 0.84), stroke (p = 0.74), and reoperation (p = 0.50). Subgroup results did not show any relevant dissimilarity.
Conclusion: The concomitant performance of LAA amputation is not associated with worse in-hospital outcomes, as measured by the composite endpoint of all-cause mortality, stroke, and reoperation.
期刊介绍:
Clinical Research in Cardiology is an international journal for clinical cardiovascular research. It provides a forum for original and review articles as well as critical perspective articles. Articles are only accepted if they meet stringent scientific standards and have undergone peer review. The journal regularly receives articles from the field of clinical cardiology, angiology, as well as heart and vascular surgery.
As the official journal of the German Cardiac Society, it gives a current and competent survey on the diagnosis and therapy of heart and vascular diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


