{"title":"日本 EGFR 基因突变阳性非小细胞肺癌的预后因素:一项真实世界单中心回顾性队列研究。","authors":"Kenta Takashima, Hiroki Wakabayashi, Yu Murakami, Atsuhito Saiki, Yasuo Matsuzawa","doi":"10.1007/s40801-024-00449-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The prognosis of patients with epidermal growth factor receptor (EGFR) mutation-positive lung cancer has improved significantly since the advent of EGFR tyrosine kinase inhibitors (EGFR-TKIs). We aimed to investigate the relationship between patient characteristics, EGFR genotype, therapeutic agents, and the prognosis of the patients with EGFR mutation-positive lung cancer.</p><p><strong>Methods: </strong>This retrospective cohort study analyzed 198 Japanese patients with unresectable EGFR mutation-positive lung cancer who were treated with EGFR-TKIs at Toho University Sakura Medical Center from April 2006 to December 2021. Factors associated with overall survival (OS) were analyzed using Cox proportional hazards analysis.</p><p><strong>Results: </strong>Patients who received osimertinib had a significantly longer OS than did those not receiving it (median OS, 36.2 versus 20.7 months; p < 0.001).There were significant differences in OS between patients with EGFR mutation who received osimertinib as first-line treatment, T790M-positive patients who received osimertinib as second- or later-line treatment, and those who did not receive it (median OS, 28.2 versus 40.2 versus 20.7 months; p = 0.003). However, in T790M-negative patients, no significant difference in OS was noted between those who did and did not receive osimertinib as post-treatment (median OS, 28.0 versus 40.0 months; p = 0.619). Multivariate Cox proportional hazards analysis showed that osimertinib treatment was associated with longer OS (hazard ratio, 0.480; 95% confidence interval, 0.326-0.707; p < 0.001).</p><p><strong>Conclusion: </strong>The patients who were T790M-positive in the first-line treatment with first or second-generation EGFR-TKIs and were given osimertinib as the second or later line treatment had a better prognosis than the patients who were T790M-negative in the first-line treatment with first or second-generation EGFR-TKIs and could not receive osimertinib.</p>","PeriodicalId":11282,"journal":{"name":"Drugs - Real World Outcomes","volume":" ","pages":"603-615"},"PeriodicalIF":1.9000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11589054/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic Factors in Japanese EGFR Mutation-Positive Non-Small-Cell Lung Cancer: A Real-World Single-Center Retrospective Cohort Study.\",\"authors\":\"Kenta Takashima, Hiroki Wakabayashi, Yu Murakami, Atsuhito Saiki, Yasuo Matsuzawa\",\"doi\":\"10.1007/s40801-024-00449-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The prognosis of patients with epidermal growth factor receptor (EGFR) mutation-positive lung cancer has improved significantly since the advent of EGFR tyrosine kinase inhibitors (EGFR-TKIs). We aimed to investigate the relationship between patient characteristics, EGFR genotype, therapeutic agents, and the prognosis of the patients with EGFR mutation-positive lung cancer.</p><p><strong>Methods: </strong>This retrospective cohort study analyzed 198 Japanese patients with unresectable EGFR mutation-positive lung cancer who were treated with EGFR-TKIs at Toho University Sakura Medical Center from April 2006 to December 2021. Factors associated with overall survival (OS) were analyzed using Cox proportional hazards analysis.</p><p><strong>Results: </strong>Patients who received osimertinib had a significantly longer OS than did those not receiving it (median OS, 36.2 versus 20.7 months; p < 0.001).There were significant differences in OS between patients with EGFR mutation who received osimertinib as first-line treatment, T790M-positive patients who received osimertinib as second- or later-line treatment, and those who did not receive it (median OS, 28.2 versus 40.2 versus 20.7 months; p = 0.003). However, in T790M-negative patients, no significant difference in OS was noted between those who did and did not receive osimertinib as post-treatment (median OS, 28.0 versus 40.0 months; p = 0.619). Multivariate Cox proportional hazards analysis showed that osimertinib treatment was associated with longer OS (hazard ratio, 0.480; 95% confidence interval, 0.326-0.707; p < 0.001).</p><p><strong>Conclusion: </strong>The patients who were T790M-positive in the first-line treatment with first or second-generation EGFR-TKIs and were given osimertinib as the second or later line treatment had a better prognosis than the patients who were T790M-negative in the first-line treatment with first or second-generation EGFR-TKIs and could not receive osimertinib.</p>\",\"PeriodicalId\":11282,\"journal\":{\"name\":\"Drugs - Real World Outcomes\",\"volume\":\" \",\"pages\":\"603-615\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11589054/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drugs - Real World Outcomes\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40801-024-00449-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs - Real World Outcomes","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40801-024-00449-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Prognostic Factors in Japanese EGFR Mutation-Positive Non-Small-Cell Lung Cancer: A Real-World Single-Center Retrospective Cohort Study.
Background: The prognosis of patients with epidermal growth factor receptor (EGFR) mutation-positive lung cancer has improved significantly since the advent of EGFR tyrosine kinase inhibitors (EGFR-TKIs). We aimed to investigate the relationship between patient characteristics, EGFR genotype, therapeutic agents, and the prognosis of the patients with EGFR mutation-positive lung cancer.
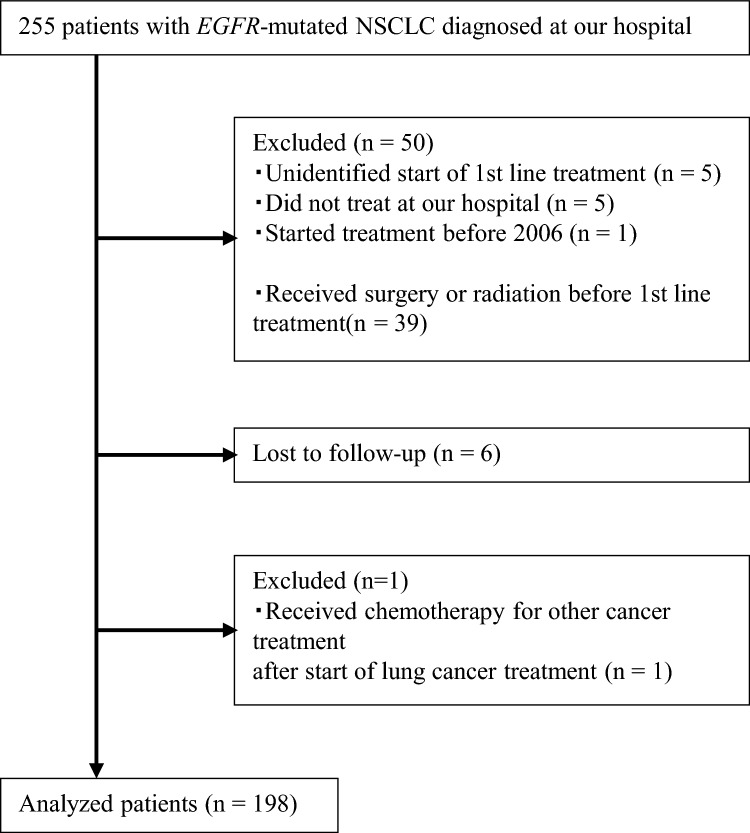
Methods: This retrospective cohort study analyzed 198 Japanese patients with unresectable EGFR mutation-positive lung cancer who were treated with EGFR-TKIs at Toho University Sakura Medical Center from April 2006 to December 2021. Factors associated with overall survival (OS) were analyzed using Cox proportional hazards analysis.
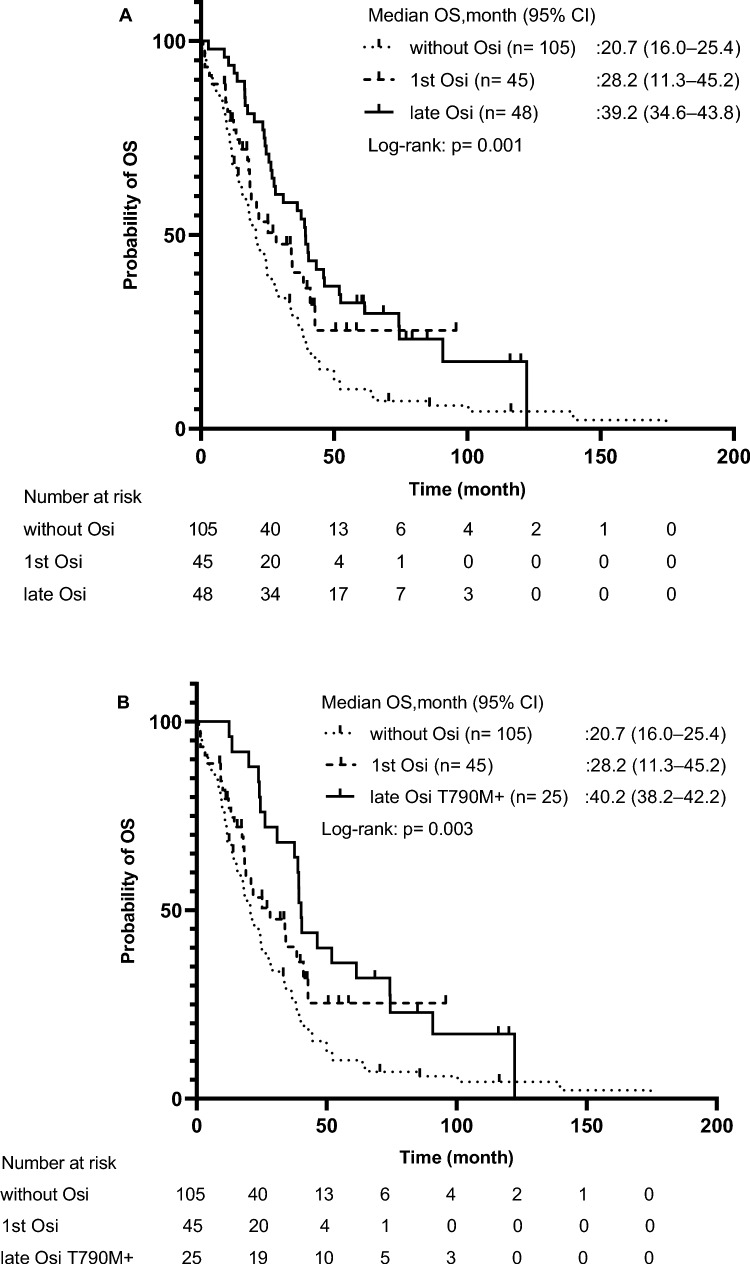
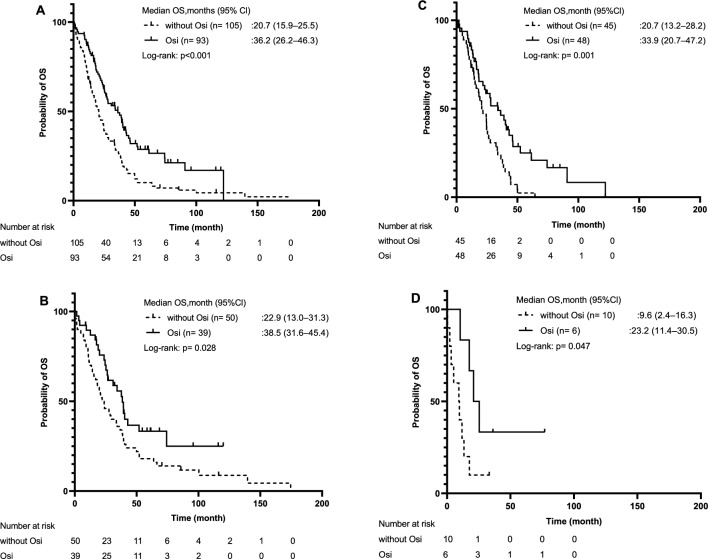
Results: Patients who received osimertinib had a significantly longer OS than did those not receiving it (median OS, 36.2 versus 20.7 months; p < 0.001).There were significant differences in OS between patients with EGFR mutation who received osimertinib as first-line treatment, T790M-positive patients who received osimertinib as second- or later-line treatment, and those who did not receive it (median OS, 28.2 versus 40.2 versus 20.7 months; p = 0.003). However, in T790M-negative patients, no significant difference in OS was noted between those who did and did not receive osimertinib as post-treatment (median OS, 28.0 versus 40.0 months; p = 0.619). Multivariate Cox proportional hazards analysis showed that osimertinib treatment was associated with longer OS (hazard ratio, 0.480; 95% confidence interval, 0.326-0.707; p < 0.001).
Conclusion: The patients who were T790M-positive in the first-line treatment with first or second-generation EGFR-TKIs and were given osimertinib as the second or later line treatment had a better prognosis than the patients who were T790M-negative in the first-line treatment with first or second-generation EGFR-TKIs and could not receive osimertinib.
期刊介绍:
Drugs - Real World Outcomes targets original research and definitive reviews regarding the use of real-world data to evaluate health outcomes and inform healthcare decision-making on drugs, devices and other interventions in clinical practice. The journal includes, but is not limited to, the following research areas: Using registries/databases/health records and other non-selected observational datasets to investigate: drug use and treatment outcomes prescription patterns drug safety signals adherence to treatment guidelines benefit : risk profiles comparative effectiveness economic analyses including cost-of-illness Data-driven research methodologies, including the capture, curation, search, sharing, analysis and interpretation of ‘big data’ Techniques and approaches to optimise real-world modelling.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


