Aimée S. R. Westerveld, Pien Roesthuis, Helena J. H. van der Pal, Dorine Bresters, Marc Bierings, Jacqueline Loonen, Andrica C. H. de Vries, Marloes Louwerens, Maria M. W. Koopman, Marry M. van den Heuvel-Eibrink, Margriet van der Heiden-van der Loo, Peter Hoogerbrugge, Geert O. Janssens, Ronald R. de Krijger, Cecile M. Ronckers, Rob Pieters, Leontien C. M. Kremer, Jop C. Teepen
{"title":"儿童急性淋巴细胞白血病 5 年存活者接受造血干细胞移植后罹患后续肿瘤的风险增加","authors":"Aimée S. R. Westerveld, Pien Roesthuis, Helena J. H. van der Pal, Dorine Bresters, Marc Bierings, Jacqueline Loonen, Andrica C. H. de Vries, Marloes Louwerens, Maria M. W. Koopman, Marry M. van den Heuvel-Eibrink, Margriet van der Heiden-van der Loo, Peter Hoogerbrugge, Geert O. Janssens, Ronald R. de Krijger, Cecile M. Ronckers, Rob Pieters, Leontien C. M. Kremer, Jop C. Teepen","doi":"10.1038/s41408-024-01122-7","DOIUrl":null,"url":null,"abstract":"<p>Acute lymphoblastic leukemia (ALL) survivors are at risk for developing subsequent neoplasms, but there is limited information on long-term risks and risk factors for both subsequent malignant neoplasms (SMNs) and subsequent non-malignant neoplasms (SNMNs). We analyzed long-term risk and risk factors for SMNs and SNMNs among 3291 5-year ALL survivors from the Dutch Childhood Cancer Survivor Study-LATER cohort (1963–2014). We calculated standardized incidence ratios (SIRs) and cumulative incidences and used multivariable Cox proportional hazard regression analyses for analyzing risk factors. A total of 97 survivors developed SMNs and 266 SNMNs. The 30-year cumulative incidence was 4.1% (95%CI: 3.5–5.3) for SMNs and 10.4%(95%CI: 8.9–12.1) for SNMNs. Risk of SMNs was elevated compared to the general population (SIR: 2.6, 95%CI: 2.1–3.1). Survivors treated with hematopoietic stem cell transplantation (HSCT) with total body irradiation (TBI) (HR:4.2, 95%CI: 2.3–7.9), and without TBI (HR:4.0,95%CI: 1.2–13.7) showed increased SMN risk versus non-transplanted survivors. Cranial radiotherapy (CRT) was also a risk factor for SMNs (HR:2.1, 95%CI: 1.4–4.0). In conclusion, childhood ALL survivors have an increased SMN risk, especially after HSCT and CRT. A key finding is that even HSCT-treated survivors without TBI treatment showed an increased SMN risk, possibly due to accompanied chemotherapy treatment. This emphasizes the need for careful follow-up of HSCT and/or CRT-treated survivors.</p>","PeriodicalId":8989,"journal":{"name":"Blood Cancer Journal","volume":"34 1","pages":""},"PeriodicalIF":11.6000,"publicationDate":"2024-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Increased risk of subsequent neoplasm after hematopoietic stem cell transplantation in 5-year survivors of childhood acute lymphoblastic leukemia\",\"authors\":\"Aimée S. R. Westerveld, Pien Roesthuis, Helena J. H. van der Pal, Dorine Bresters, Marc Bierings, Jacqueline Loonen, Andrica C. H. de Vries, Marloes Louwerens, Maria M. W. Koopman, Marry M. van den Heuvel-Eibrink, Margriet van der Heiden-van der Loo, Peter Hoogerbrugge, Geert O. Janssens, Ronald R. de Krijger, Cecile M. Ronckers, Rob Pieters, Leontien C. M. Kremer, Jop C. Teepen\",\"doi\":\"10.1038/s41408-024-01122-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Acute lymphoblastic leukemia (ALL) survivors are at risk for developing subsequent neoplasms, but there is limited information on long-term risks and risk factors for both subsequent malignant neoplasms (SMNs) and subsequent non-malignant neoplasms (SNMNs). We analyzed long-term risk and risk factors for SMNs and SNMNs among 3291 5-year ALL survivors from the Dutch Childhood Cancer Survivor Study-LATER cohort (1963–2014). We calculated standardized incidence ratios (SIRs) and cumulative incidences and used multivariable Cox proportional hazard regression analyses for analyzing risk factors. A total of 97 survivors developed SMNs and 266 SNMNs. The 30-year cumulative incidence was 4.1% (95%CI: 3.5–5.3) for SMNs and 10.4%(95%CI: 8.9–12.1) for SNMNs. Risk of SMNs was elevated compared to the general population (SIR: 2.6, 95%CI: 2.1–3.1). Survivors treated with hematopoietic stem cell transplantation (HSCT) with total body irradiation (TBI) (HR:4.2, 95%CI: 2.3–7.9), and without TBI (HR:4.0,95%CI: 1.2–13.7) showed increased SMN risk versus non-transplanted survivors. Cranial radiotherapy (CRT) was also a risk factor for SMNs (HR:2.1, 95%CI: 1.4–4.0). In conclusion, childhood ALL survivors have an increased SMN risk, especially after HSCT and CRT. A key finding is that even HSCT-treated survivors without TBI treatment showed an increased SMN risk, possibly due to accompanied chemotherapy treatment. This emphasizes the need for careful follow-up of HSCT and/or CRT-treated survivors.</p>\",\"PeriodicalId\":8989,\"journal\":{\"name\":\"Blood Cancer Journal\",\"volume\":\"34 1\",\"pages\":\"\"},\"PeriodicalIF\":11.6000,\"publicationDate\":\"2024-08-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood Cancer Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41408-024-01122-7\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Cancer Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41408-024-01122-7","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
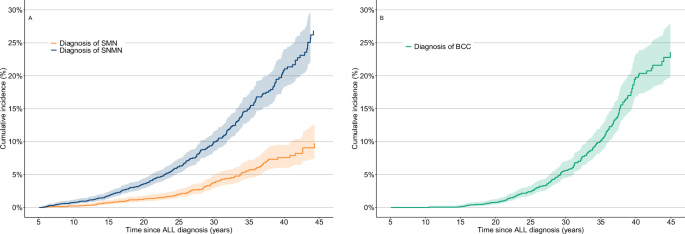
急性淋巴细胞白血病(ALL)幸存者有罹患后续肿瘤的风险,但关于后续恶性肿瘤(SMN)和后续非恶性肿瘤(SNMN)的长期风险和风险因素的信息却很有限。我们分析了荷兰儿童癌症幸存者研究(Dutch Childhood Cancer Survivor Study-LATER)队列(1963-2014)中 3291 名 5 年期 ALL 幸存者罹患 SMNs 和 SNMNs 的长期风险和风险因素。我们计算了标准化发病率(SIR)和累积发病率,并使用多变量考克斯比例危险回归分析法分析了风险因素。共有 97 名幸存者罹患 SMN,266 名幸存者罹患 SNMN。SMN和SNMN的30年累积发病率分别为4.1%(95%CI:3.5-5.3)和10.4%(95%CI:8.9-12.1)。与普通人群相比,SMNs 的风险较高(SIR:2.6,95%CI:2.1-3.1)。接受造血干细胞移植(HSCT)并全身照射(TBI)(HR:4.2,95%CI:2.3-7.9)和未接受TBI(HR:4.0,95%CI:1.2-13.7)的幸存者与未接受移植的幸存者相比,SMN风险增加。颅脑放疗(CRT)也是SMN的一个风险因素(HR:2.1,95%CI:1.4-4.0)。总之,儿童 ALL 存活者 SMN 风险增加,尤其是造血干细胞移植和 CRT 后。一个重要发现是,即使造血干细胞移植后的幸存者未接受过创伤性脑损伤治疗,其SMN风险也会增加,这可能是由于伴随化疗所致。这强调了对造血干细胞移植和/或 CRT 治疗幸存者进行仔细随访的必要性。
Increased risk of subsequent neoplasm after hematopoietic stem cell transplantation in 5-year survivors of childhood acute lymphoblastic leukemia
Acute lymphoblastic leukemia (ALL) survivors are at risk for developing subsequent neoplasms, but there is limited information on long-term risks and risk factors for both subsequent malignant neoplasms (SMNs) and subsequent non-malignant neoplasms (SNMNs). We analyzed long-term risk and risk factors for SMNs and SNMNs among 3291 5-year ALL survivors from the Dutch Childhood Cancer Survivor Study-LATER cohort (1963–2014). We calculated standardized incidence ratios (SIRs) and cumulative incidences and used multivariable Cox proportional hazard regression analyses for analyzing risk factors. A total of 97 survivors developed SMNs and 266 SNMNs. The 30-year cumulative incidence was 4.1% (95%CI: 3.5–5.3) for SMNs and 10.4%(95%CI: 8.9–12.1) for SNMNs. Risk of SMNs was elevated compared to the general population (SIR: 2.6, 95%CI: 2.1–3.1). Survivors treated with hematopoietic stem cell transplantation (HSCT) with total body irradiation (TBI) (HR:4.2, 95%CI: 2.3–7.9), and without TBI (HR:4.0,95%CI: 1.2–13.7) showed increased SMN risk versus non-transplanted survivors. Cranial radiotherapy (CRT) was also a risk factor for SMNs (HR:2.1, 95%CI: 1.4–4.0). In conclusion, childhood ALL survivors have an increased SMN risk, especially after HSCT and CRT. A key finding is that even HSCT-treated survivors without TBI treatment showed an increased SMN risk, possibly due to accompanied chemotherapy treatment. This emphasizes the need for careful follow-up of HSCT and/or CRT-treated survivors.
期刊介绍:
Blood Cancer Journal is dedicated to publishing high-quality articles related to hematologic malignancies and related disorders. The journal welcomes submissions of original research, reviews, guidelines, and letters that are deemed to have a significant impact in the field. While the journal covers a wide range of topics, it particularly focuses on areas such as:
Preclinical studies of new compounds, especially those that provide mechanistic insights
Clinical trials and observations
Reviews related to new drugs and current management of hematologic malignancies
Novel observations related to new mutations, molecular pathways, and tumor genomics
Blood Cancer Journal offers a forum for expedited publication of novel observations regarding new mutations or altered pathways.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


