Janet Bondarenko, Simone Dal Corso, Michael P Dillon, Sally Singh, Belinda R Miller, Caroline Kein, Anne E Holland, Arwel W Jones
{"title":"慢性呼吸系统疾病患者在中心或家庭进行肺康复治疗后的临床重要变化和不良事件:系统回顾和荟萃分析。","authors":"Janet Bondarenko, Simone Dal Corso, Michael P Dillon, Sally Singh, Belinda R Miller, Caroline Kein, Anne E Holland, Arwel W Jones","doi":"10.1177/14799731241277808","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objectives:</b> To determine the proportion of people who achieve minimal clinically important differences (MCID) with centre-based or home-based pulmonary rehabilitation and to synthesise data on adverse events.<b>Methods:</b> Cochrane reviews and electronic databases were searched to identify randomised trials comparing centre-based to home-based pulmonary rehabilitation, or either model to usual care, in people with chronic respiratory disease. Primary outcomes were the proportion of participants achieving MCIDs in exercise capacity and disease-specific quality of life. Secondary outcomes were symptoms and adverse events. Cochrane Risk of Bias 1.0 and GRADE were used to assess the risk of bias and certainty of evidence respectively.<b>Results:</b> Forty-nine trials were eligible. Compared to usual care, a higher proportion of pulmonary rehabilitation participants achieved the MCID for exercise capacity (6MWT: 47% vs 20%, <i>p</i> = 0.11), dyspnoea (43% vs 29%, <i>p</i> = 0.0001), fatigue (48% vs 27%, <i>p</i> = 0.0002) and emotional function (37% vs 25%, <i>p</i> = 0.02), with all of these between group differences statistically significant except for exercise capacity. There were no differences between centre-based and home-based pulmonary rehabilitation in the proportion of participants who achieved MCIDs (34%- 58% across studies). Ninety percent of trials reported no adverse events. Certainty of evidence was low-to- moderate with all outcomes except for CRQ-mastery (centre-based vs home-based pulmonary rehabilitation, or pulmonary rehabilitation vs usual care in COPD), ESWT (pulmonary rehabilitation vs usual care in COPD) and 6MWT (pulmonary rehabilitation vs usual care in bronchiectasis) where evidence was very uncertain.<b>Discussion:</b> Clinically meaningful outcomes are achieved by similar proportions of participants in centre-based and home-based pulmonary rehabilitation, with few adverse events. Reporting of trial outcomes according to MCIDs is necessary for informed decision making regarding pulmonary rehabilitation models.</p>","PeriodicalId":10217,"journal":{"name":"Chronic Respiratory Disease","volume":"21 ","pages":"14799731241277808"},"PeriodicalIF":2.3000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11348370/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinically important changes and adverse events with centre-based or home-based pulmonary rehabilitation in chronic respiratory disease: A systematic review and meta-analysis.\",\"authors\":\"Janet Bondarenko, Simone Dal Corso, Michael P Dillon, Sally Singh, Belinda R Miller, Caroline Kein, Anne E Holland, Arwel W Jones\",\"doi\":\"10.1177/14799731241277808\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Objectives:</b> To determine the proportion of people who achieve minimal clinically important differences (MCID) with centre-based or home-based pulmonary rehabilitation and to synthesise data on adverse events.<b>Methods:</b> Cochrane reviews and electronic databases were searched to identify randomised trials comparing centre-based to home-based pulmonary rehabilitation, or either model to usual care, in people with chronic respiratory disease. Primary outcomes were the proportion of participants achieving MCIDs in exercise capacity and disease-specific quality of life. Secondary outcomes were symptoms and adverse events. Cochrane Risk of Bias 1.0 and GRADE were used to assess the risk of bias and certainty of evidence respectively.<b>Results:</b> Forty-nine trials were eligible. Compared to usual care, a higher proportion of pulmonary rehabilitation participants achieved the MCID for exercise capacity (6MWT: 47% vs 20%, <i>p</i> = 0.11), dyspnoea (43% vs 29%, <i>p</i> = 0.0001), fatigue (48% vs 27%, <i>p</i> = 0.0002) and emotional function (37% vs 25%, <i>p</i> = 0.02), with all of these between group differences statistically significant except for exercise capacity. There were no differences between centre-based and home-based pulmonary rehabilitation in the proportion of participants who achieved MCIDs (34%- 58% across studies). Ninety percent of trials reported no adverse events. Certainty of evidence was low-to- moderate with all outcomes except for CRQ-mastery (centre-based vs home-based pulmonary rehabilitation, or pulmonary rehabilitation vs usual care in COPD), ESWT (pulmonary rehabilitation vs usual care in COPD) and 6MWT (pulmonary rehabilitation vs usual care in bronchiectasis) where evidence was very uncertain.<b>Discussion:</b> Clinically meaningful outcomes are achieved by similar proportions of participants in centre-based and home-based pulmonary rehabilitation, with few adverse events. Reporting of trial outcomes according to MCIDs is necessary for informed decision making regarding pulmonary rehabilitation models.</p>\",\"PeriodicalId\":10217,\"journal\":{\"name\":\"Chronic Respiratory Disease\",\"volume\":\"21 \",\"pages\":\"14799731241277808\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11348370/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Chronic Respiratory Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/14799731241277808\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14799731241277808","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
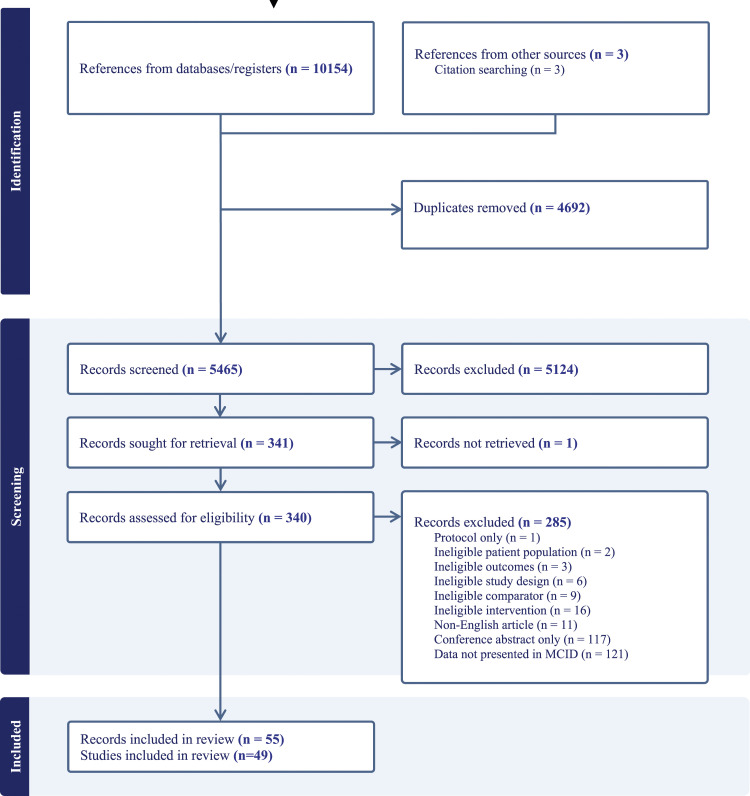
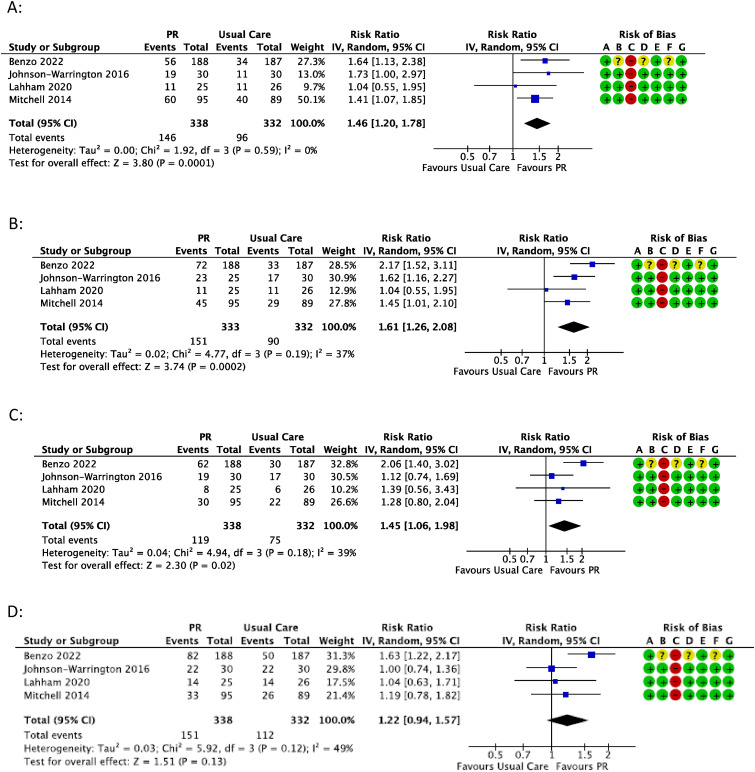
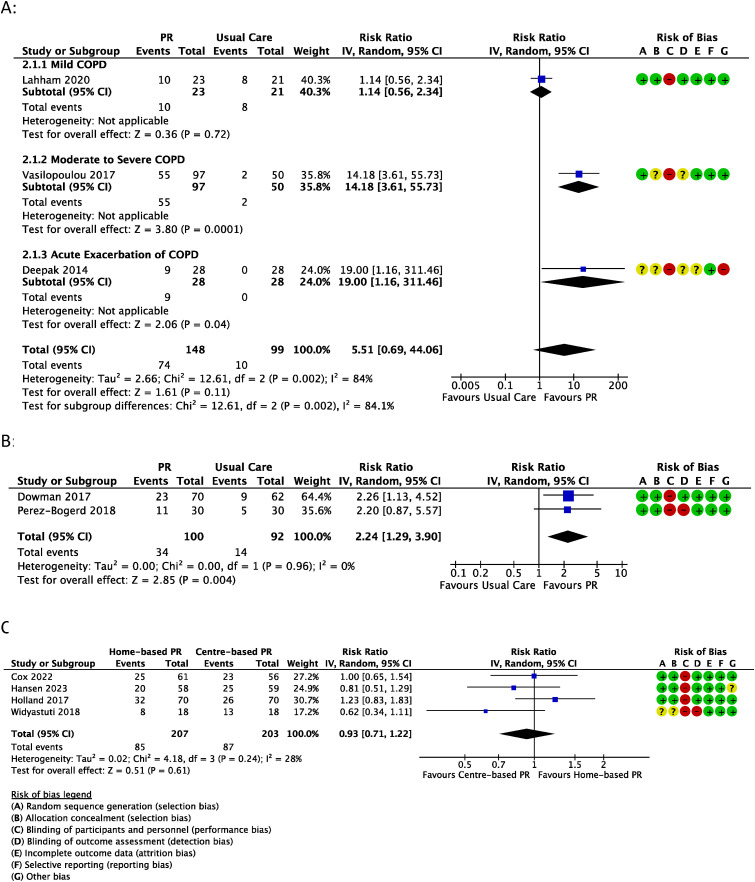
目的确定在中心或家庭肺康复治疗中达到最小临床重要差异(MCID)的人数比例,并对不良事件数据进行综合分析:方法: 对 Cochrane 综述和电子数据库进行检索,以确定在慢性呼吸系统疾病患者中比较中心型肺康复与家庭型肺康复或其中一种模式与常规护理的随机试验。主要结果为达到运动能力和疾病特异性生活质量 MCID 的参与者比例。次要结果是症状和不良事件。Cochrane Risk of Bias 1.0 和 GRADE 分别用于评估偏倚风险和证据的确定性:49项试验符合条件。与常规护理相比,肺康复参与者在运动能力(6MWT:47% vs 20%,p = 0.11)、呼吸困难(43% vs 29%,p = 0.0001)、疲劳(48% vs 27%,p = 0.0002)和情绪功能(37% vs 25%,p = 0.02)方面达到MCID的比例更高,除运动能力外,所有这些组间差异均有统计学意义。在达到 MCID 的参与者比例方面,中心康复和家庭康复没有差异(各研究中的比例从 34% 到 58%)。90%的试验未报告不良事件。除CRQ-mastery(中心康复与家庭康复,或肺康复与慢性阻塞性肺病常规护理)、ESWT(肺康复与慢性阻塞性肺病常规护理)和6MWT(肺康复与支气管扩张症常规护理)的证据非常不确定外,其他所有结果的证据确定性均为中低:讨论:在中心和家庭肺康复治疗中,获得有临床意义结果的参与者比例相似,且不良事件较少。根据MCIDs报告试验结果对于肺康复模式的知情决策十分必要。
Clinically important changes and adverse events with centre-based or home-based pulmonary rehabilitation in chronic respiratory disease: A systematic review and meta-analysis.
Objectives: To determine the proportion of people who achieve minimal clinically important differences (MCID) with centre-based or home-based pulmonary rehabilitation and to synthesise data on adverse events.Methods: Cochrane reviews and electronic databases were searched to identify randomised trials comparing centre-based to home-based pulmonary rehabilitation, or either model to usual care, in people with chronic respiratory disease. Primary outcomes were the proportion of participants achieving MCIDs in exercise capacity and disease-specific quality of life. Secondary outcomes were symptoms and adverse events. Cochrane Risk of Bias 1.0 and GRADE were used to assess the risk of bias and certainty of evidence respectively.Results: Forty-nine trials were eligible. Compared to usual care, a higher proportion of pulmonary rehabilitation participants achieved the MCID for exercise capacity (6MWT: 47% vs 20%, p = 0.11), dyspnoea (43% vs 29%, p = 0.0001), fatigue (48% vs 27%, p = 0.0002) and emotional function (37% vs 25%, p = 0.02), with all of these between group differences statistically significant except for exercise capacity. There were no differences between centre-based and home-based pulmonary rehabilitation in the proportion of participants who achieved MCIDs (34%- 58% across studies). Ninety percent of trials reported no adverse events. Certainty of evidence was low-to- moderate with all outcomes except for CRQ-mastery (centre-based vs home-based pulmonary rehabilitation, or pulmonary rehabilitation vs usual care in COPD), ESWT (pulmonary rehabilitation vs usual care in COPD) and 6MWT (pulmonary rehabilitation vs usual care in bronchiectasis) where evidence was very uncertain.Discussion: Clinically meaningful outcomes are achieved by similar proportions of participants in centre-based and home-based pulmonary rehabilitation, with few adverse events. Reporting of trial outcomes according to MCIDs is necessary for informed decision making regarding pulmonary rehabilitation models.
期刊介绍:
Chronic Respiratory Disease is a peer-reviewed, open access, scholarly journal, created in response to the rising incidence of chronic respiratory diseases worldwide. It publishes high quality research papers and original articles that have immediate relevance to clinical practice and its multi-disciplinary perspective reflects the nature of modern treatment. The journal provides a high quality, multi-disciplinary focus for the publication of original papers, reviews and commentary in the broad area of chronic respiratory disease, particularly its treatment and management.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


