Katherine M. Hunold MD, MPH, Lorraine C. Mion PhD, RN, FAAN, Tanya R. Gure MD, Andrew L. Schwaderer MD, Matthew Exline MD, MPH, Courtney Hebert MD, MS, Brent C. Lampert DO, Lauren T. Southerland MD, Julie A. Stephens MS, Edward W. Boyer MD, PhD, Michael Hill RN, Ching-Min B. Chu BS, Carson Reider PhD, Jeffrey M. Caterino MD, MPH
{"title":"老年急诊患者肺炎现有诊断标准的临床表现:前瞻性队列研究。","authors":"Katherine M. Hunold MD, MPH, Lorraine C. Mion PhD, RN, FAAN, Tanya R. Gure MD, Andrew L. Schwaderer MD, Matthew Exline MD, MPH, Courtney Hebert MD, MS, Brent C. Lampert DO, Lauren T. Southerland MD, Julie A. Stephens MS, Edward W. Boyer MD, PhD, Michael Hill RN, Ching-Min B. Chu BS, Carson Reider PhD, Jeffrey M. Caterino MD, MPH","doi":"10.1111/jgs.19113","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Pneumonia accounts for over half a million older adult emergency department (ED) visits annually, but ED pneumonia diagnosis is inaccurate. Geriatric-specific pneumonia diagnostic criteria exist for other settings; no prospective data exist to determine if application in the older adult ED population is feasible. The objective was to prospectively evaluate the utility of four current diagnostic criteria (Loeb; Modified McGeer; Infectious Disease Society of America/American Thoracic Society; American College of Emergency Physicians) in older adult ED patients.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This was a prospective, observational cohort study of older adult ED patients ≥65 years of age in two U.S. EDs with suspected pneumonia defined as having chest radiography ordered and treating physician suspicion. The standard we used for defining the presence, absence, or inability to determine a diagnosis of pneumonia diagnosis was expert physician chart adjudication. We report the summary statistics for demographic characteristics and symptoms/exam findings and sensitivity, specificity, and likelihood ratios with 95% confidence intervals of the existing diagnostic criteria. Pre-specified cutoff values of a positive LR >10 and a negative LR <0.3 were considered clinically significant.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 135 patients enrolled, 27 had pneumonia by adjudicator review. Typical patient-reported pneumonia symptoms, such as fever (18.5%) and new/worse cough (51.9%), were not consistently present in pneumonia. The IDSA/ATS and ACEP criteria had positive LR >10 and negative LR <0.3; however, all confidence intervals included pre-specified cutoffs.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Older adults presented to the ED with low frequency of typical pneumonia symptoms. Although existing diagnostic definitions had promising test characteristics, they may not perform well enough for clinical application without refinement.</p>\n </section>\n </div>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 10","pages":"3068-3077"},"PeriodicalIF":4.3000,"publicationDate":"2024-08-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19113","citationCount":"0","resultStr":"{\"title\":\"Clinical performance of existing diagnostic criteria for pneumonia in older emergency patients: A prospective cohort study\",\"authors\":\"Katherine M. Hunold MD, MPH, Lorraine C. Mion PhD, RN, FAAN, Tanya R. Gure MD, Andrew L. Schwaderer MD, Matthew Exline MD, MPH, Courtney Hebert MD, MS, Brent C. Lampert DO, Lauren T. Southerland MD, Julie A. Stephens MS, Edward W. Boyer MD, PhD, Michael Hill RN, Ching-Min B. Chu BS, Carson Reider PhD, Jeffrey M. Caterino MD, MPH\",\"doi\":\"10.1111/jgs.19113\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Pneumonia accounts for over half a million older adult emergency department (ED) visits annually, but ED pneumonia diagnosis is inaccurate. Geriatric-specific pneumonia diagnostic criteria exist for other settings; no prospective data exist to determine if application in the older adult ED population is feasible. The objective was to prospectively evaluate the utility of four current diagnostic criteria (Loeb; Modified McGeer; Infectious Disease Society of America/American Thoracic Society; American College of Emergency Physicians) in older adult ED patients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This was a prospective, observational cohort study of older adult ED patients ≥65 years of age in two U.S. EDs with suspected pneumonia defined as having chest radiography ordered and treating physician suspicion. The standard we used for defining the presence, absence, or inability to determine a diagnosis of pneumonia diagnosis was expert physician chart adjudication. We report the summary statistics for demographic characteristics and symptoms/exam findings and sensitivity, specificity, and likelihood ratios with 95% confidence intervals of the existing diagnostic criteria. Pre-specified cutoff values of a positive LR >10 and a negative LR <0.3 were considered clinically significant.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 135 patients enrolled, 27 had pneumonia by adjudicator review. Typical patient-reported pneumonia symptoms, such as fever (18.5%) and new/worse cough (51.9%), were not consistently present in pneumonia. The IDSA/ATS and ACEP criteria had positive LR >10 and negative LR <0.3; however, all confidence intervals included pre-specified cutoffs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Older adults presented to the ED with low frequency of typical pneumonia symptoms. Although existing diagnostic definitions had promising test characteristics, they may not perform well enough for clinical application without refinement.</p>\\n </section>\\n </div>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"72 10\",\"pages\":\"3068-3077\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-08-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19113\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19113\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19113","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:每年有 50 多万老年人因肺炎到急诊科(ED)就诊,但急诊科肺炎诊断并不准确。目前已有针对其他环境的老年肺炎诊断标准,但尚无前瞻性数据来确定在老年人急诊室人群中应用这些标准是否可行。我们的目的是前瞻性地评估目前四种诊断标准(Loeb、修订版 McGeer、美国传染病学会/美国胸科学会、美国急诊医师学会)在老年急诊室患者中的实用性:这是一项前瞻性的观察性队列研究,研究对象是美国两家急诊室中年龄≥65 岁的老年急诊患者,其疑似肺炎的定义是已接受胸片检查且主治医生怀疑其患有肺炎。我们采用专家医师的病历判定标准来界定是否存在肺炎诊断或无法确定肺炎诊断。我们报告了现有诊断标准的人口统计学特征、症状/检查结果、灵敏度、特异性、似然比及 95% 置信区间的汇总统计。预设的临界值为阳性 LR >10 和阴性 LR 结果:在 135 名入选患者中,经评审员审查,27 人患有肺炎。患者报告的典型肺炎症状,如发热(18.5%)和新发/加重的咳嗽(51.9%),在肺炎中并不总是出现。IDSA/ATS 和 ACEP 标准的阳性 LR >10 和阴性 LR 结论:老年人在急诊室出现典型肺炎症状的频率较低。虽然现有的诊断定义具有很好的测试特性,但如果不加以改进,它们可能无法很好地应用于临床。
Clinical performance of existing diagnostic criteria for pneumonia in older emergency patients: A prospective cohort study
Background
Pneumonia accounts for over half a million older adult emergency department (ED) visits annually, but ED pneumonia diagnosis is inaccurate. Geriatric-specific pneumonia diagnostic criteria exist for other settings; no prospective data exist to determine if application in the older adult ED population is feasible. The objective was to prospectively evaluate the utility of four current diagnostic criteria (Loeb; Modified McGeer; Infectious Disease Society of America/American Thoracic Society; American College of Emergency Physicians) in older adult ED patients.
Methods
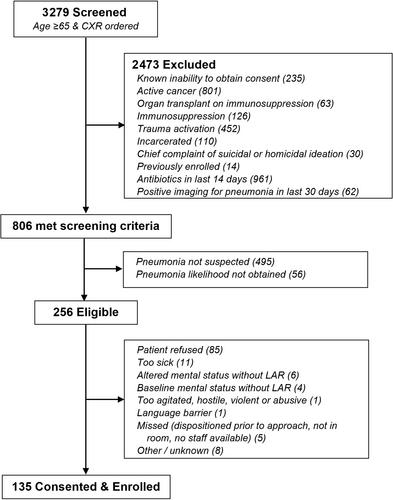
This was a prospective, observational cohort study of older adult ED patients ≥65 years of age in two U.S. EDs with suspected pneumonia defined as having chest radiography ordered and treating physician suspicion. The standard we used for defining the presence, absence, or inability to determine a diagnosis of pneumonia diagnosis was expert physician chart adjudication. We report the summary statistics for demographic characteristics and symptoms/exam findings and sensitivity, specificity, and likelihood ratios with 95% confidence intervals of the existing diagnostic criteria. Pre-specified cutoff values of a positive LR >10 and a negative LR <0.3 were considered clinically significant.
Results
Of 135 patients enrolled, 27 had pneumonia by adjudicator review. Typical patient-reported pneumonia symptoms, such as fever (18.5%) and new/worse cough (51.9%), were not consistently present in pneumonia. The IDSA/ATS and ACEP criteria had positive LR >10 and negative LR <0.3; however, all confidence intervals included pre-specified cutoffs.
Conclusions
Older adults presented to the ED with low frequency of typical pneumonia symptoms. Although existing diagnostic definitions had promising test characteristics, they may not perform well enough for clinical application without refinement.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


