{"title":"引产或催产是否会影响鞘内阿片类药物的镇痛效果?回顾性队列研究","authors":"Lotta Salmi, Riina Jernman, Antti Väänänen","doi":"10.1155/2024/6647974","DOIUrl":null,"url":null,"abstract":"<div>\n <p><i>Background</i>. Induction or augmentation of labor may cause more painful contractions compared to spontaneous labor and pose a challenge to the efficacy of analgesia provided by spinal opioids alone in the early phase of labor. Therefore, we studied the analgesic efficacy and maternal satisfaction during spontaneous and artificially induced or augmented delivery in parturients receiving neuraxial analgesia with intrathecal opioids. <i>Methods</i>. A forty-parturient cohort that received intrathecal opioid (sufentanil 5 <i>µ</i>g or fentanyl 20 <i>µ</i>g) by the combined spinal-epidural method at an early phase of labor (cervical dilatation ≤5 cm) was used for this post hoc study. Maternal satisfaction and pain during contractions were measured on 0–100 visual analog scale at 30 minutes after the initiation of labor analgesia. Obstetric parameters (methods used to advance labor, cervical dilatation, use of oxytocin, effective time of spinal opioids, and labor outcome) were also measured. <i>Results</i>. Of the 40 parturients, 18 had spontaneous labor and 22 had induced or augmented labor (prior cervical dilatation, artificial rupture of membranes, or oxytocin infusion at the time of neuraxial analgesia initiation). Spontaneous labor associated with lower mean pain scores (6.4 (±12.8) vs 29.6 (±30.6) mm, <i>P</i> = 0.005) and higher satisfaction scores (96.9 (±5.3) vs 81.1 (±28.0) mm, <i>P</i> = 0.024) compared to induced or oxytocin augmented labor at 30 minutes after the initiation of analgesia. The parturients were at a similar stage of labor, and their labor progressed at a similar rate. <i>Conclusions</i>. In parturients undergoing nonspontaneous labor, the initiation of labor analgesia by intrathecal opioids alone may not be sufficient for adequate analgesia and either intrathecal or epidural analgesia with a mixture of opioid and local anesthetic should be considered in this population. This trial is registered with NCT02885350.</p>\n </div>","PeriodicalId":15381,"journal":{"name":"Journal of Clinical Pharmacy and Therapeutics","volume":"2024 1","pages":""},"PeriodicalIF":2.0000,"publicationDate":"2024-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/6647974","citationCount":"0","resultStr":"{\"title\":\"Does Induction or Augmentation of Labor Affect the Analgesic Efficacy of Intrathecal Opioids?: A Retrospective Cohort Study\",\"authors\":\"Lotta Salmi, Riina Jernman, Antti Väänänen\",\"doi\":\"10.1155/2024/6647974\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n <p><i>Background</i>. Induction or augmentation of labor may cause more painful contractions compared to spontaneous labor and pose a challenge to the efficacy of analgesia provided by spinal opioids alone in the early phase of labor. Therefore, we studied the analgesic efficacy and maternal satisfaction during spontaneous and artificially induced or augmented delivery in parturients receiving neuraxial analgesia with intrathecal opioids. <i>Methods</i>. A forty-parturient cohort that received intrathecal opioid (sufentanil 5 <i>µ</i>g or fentanyl 20 <i>µ</i>g) by the combined spinal-epidural method at an early phase of labor (cervical dilatation ≤5 cm) was used for this post hoc study. Maternal satisfaction and pain during contractions were measured on 0–100 visual analog scale at 30 minutes after the initiation of labor analgesia. Obstetric parameters (methods used to advance labor, cervical dilatation, use of oxytocin, effective time of spinal opioids, and labor outcome) were also measured. <i>Results</i>. Of the 40 parturients, 18 had spontaneous labor and 22 had induced or augmented labor (prior cervical dilatation, artificial rupture of membranes, or oxytocin infusion at the time of neuraxial analgesia initiation). Spontaneous labor associated with lower mean pain scores (6.4 (±12.8) vs 29.6 (±30.6) mm, <i>P</i> = 0.005) and higher satisfaction scores (96.9 (±5.3) vs 81.1 (±28.0) mm, <i>P</i> = 0.024) compared to induced or oxytocin augmented labor at 30 minutes after the initiation of analgesia. The parturients were at a similar stage of labor, and their labor progressed at a similar rate. <i>Conclusions</i>. In parturients undergoing nonspontaneous labor, the initiation of labor analgesia by intrathecal opioids alone may not be sufficient for adequate analgesia and either intrathecal or epidural analgesia with a mixture of opioid and local anesthetic should be considered in this population. This trial is registered with NCT02885350.</p>\\n </div>\",\"PeriodicalId\":15381,\"journal\":{\"name\":\"Journal of Clinical Pharmacy and Therapeutics\",\"volume\":\"2024 1\",\"pages\":\"\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2024-08-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/6647974\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Pharmacy and Therapeutics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1155/2024/6647974\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Pharmacy and Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/6647974","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Does Induction or Augmentation of Labor Affect the Analgesic Efficacy of Intrathecal Opioids?: A Retrospective Cohort Study
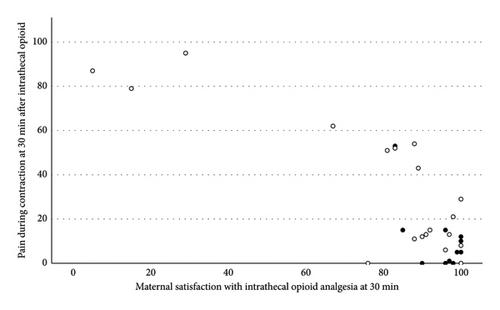
Background. Induction or augmentation of labor may cause more painful contractions compared to spontaneous labor and pose a challenge to the efficacy of analgesia provided by spinal opioids alone in the early phase of labor. Therefore, we studied the analgesic efficacy and maternal satisfaction during spontaneous and artificially induced or augmented delivery in parturients receiving neuraxial analgesia with intrathecal opioids. Methods. A forty-parturient cohort that received intrathecal opioid (sufentanil 5 µg or fentanyl 20 µg) by the combined spinal-epidural method at an early phase of labor (cervical dilatation ≤5 cm) was used for this post hoc study. Maternal satisfaction and pain during contractions were measured on 0–100 visual analog scale at 30 minutes after the initiation of labor analgesia. Obstetric parameters (methods used to advance labor, cervical dilatation, use of oxytocin, effective time of spinal opioids, and labor outcome) were also measured. Results. Of the 40 parturients, 18 had spontaneous labor and 22 had induced or augmented labor (prior cervical dilatation, artificial rupture of membranes, or oxytocin infusion at the time of neuraxial analgesia initiation). Spontaneous labor associated with lower mean pain scores (6.4 (±12.8) vs 29.6 (±30.6) mm, P = 0.005) and higher satisfaction scores (96.9 (±5.3) vs 81.1 (±28.0) mm, P = 0.024) compared to induced or oxytocin augmented labor at 30 minutes after the initiation of analgesia. The parturients were at a similar stage of labor, and their labor progressed at a similar rate. Conclusions. In parturients undergoing nonspontaneous labor, the initiation of labor analgesia by intrathecal opioids alone may not be sufficient for adequate analgesia and either intrathecal or epidural analgesia with a mixture of opioid and local anesthetic should be considered in this population. This trial is registered with NCT02885350.
期刊介绍:
The Journal of Clinical Pharmacy and Therapeutics provides a forum for clinicians, pharmacists and pharmacologists to explore and report on issues of common interest. Reports and commentaries on current issues in medical and pharmaceutical practice are encouraged. Papers on evidence-based clinical practice and multidisciplinary collaborative work are particularly welcome. Regular sections in the journal include: editorials, commentaries, reviews (including systematic overviews and meta-analyses), original research and reports, and book reviews. Its scope embraces all aspects of clinical drug development and therapeutics, including:
Rational therapeutics
Evidence-based practice
Safety, cost-effectiveness and clinical efficacy of drugs
Drug interactions
Clinical impact of drug formulations
Pharmacogenetics
Personalised, stratified and translational medicine
Clinical pharmacokinetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


