Aldostefano Porcari, Ambra Masi, Ana Martinez-Naharro, Yousuf Razvi, Rishi Patel, Adam Ioannou, Muhammad U Rauf, Giulio Sinigiani, Brendan Wisniowski, Stefano Filisetti, Jasmine Currie-Cathey, Sophie O'Beara, Tushar Kotecha, Dan Knight, James C Moon, Gianfranco Sinagra, Ruta Virsinskaite, Janet Gilbertson, Lucia Venneri, Aviva Petrie, Helen Lachmann, Carol Whelan, Peter Kellman, Sriram Ravichandran, Oliver Cohen, Shameem Mahmood, Charlotte Manisty, Philip N Hawkins, Julian D Gillmore, Ashutosh D Wechalekar, Marianna Fontana
{"title":"重新定义全身性免疫球蛋白 AL 淀粉样变性的心脏受累情况和治疗目标。","authors":"Aldostefano Porcari, Ambra Masi, Ana Martinez-Naharro, Yousuf Razvi, Rishi Patel, Adam Ioannou, Muhammad U Rauf, Giulio Sinigiani, Brendan Wisniowski, Stefano Filisetti, Jasmine Currie-Cathey, Sophie O'Beara, Tushar Kotecha, Dan Knight, James C Moon, Gianfranco Sinagra, Ruta Virsinskaite, Janet Gilbertson, Lucia Venneri, Aviva Petrie, Helen Lachmann, Carol Whelan, Peter Kellman, Sriram Ravichandran, Oliver Cohen, Shameem Mahmood, Charlotte Manisty, Philip N Hawkins, Julian D Gillmore, Ashutosh D Wechalekar, Marianna Fontana","doi":"10.1001/jamacardio.2024.2555","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Cardiac amyloid infiltration is the key determinant of survival in systemic light-chain (AL) amyloidosis. Current guidelines recommend early switching therapy in patients with a nonoptimal or suboptimal response regardless of the extent of cardiac amyloid infiltration.</p><p><strong>Objective: </strong>To assess the differences between serum biomarkers, echocardiography, and cardiovascular magnetic resonance (CMR) with extracellular volume (ECV) mapping in characterizing cardiac amyloid, the independent prognostic role of these approaches, and the role of ECV mapping to guide treatment strategies.</p><p><strong>Design, setting, and participants: </strong>Consecutive patients newly diagnosed with systemic AL amyloidosis (2015-2021) underwent echocardiography, cardiac biomarkers, and CMR with ECV mapping at diagnosis. Data were analyzed from January to June 2024.</p><p><strong>Main outcomes and measures: </strong>The primary outcomes of the study were all-cause mortality and hematological response as defined according to validated criteria: no response (NR), partial response (PR), very good partial response (VGPR), and complete response (CR). Secondary outcomes were the depth and speed of hematological response and overall survival according to ECV.</p><p><strong>Results: </strong>Of 560 patients with AL amyloidosis, the median (IQR) age was 68 years (59-74 years); 346 patients were male (61.8%) and 214 female (38.2%). Over a median (IQR) 40.5 months 9-58 months), ECV was independently associated with mortality. In the landmark analysis at 1 month, long-term survival was independent of the achieved hematological response in ECV less than 0.30% and ECV of 0.31% to 0.40%, while it was dependent on the depth of the hematological response in ECV greater than 0.40%. In the landmark analysis at 6 months, survival was independent of the achieved hematological response in ECV less than 0.30% and dependent on achieving at least PR in ECV of 0.31% to 0.40%. Survival was dependent on achieving CR in ECV of 0.41% to 0.50% and ECV greater than 0.50%. Achieving a deep hematological response at 1 month was associated with better survival compared with 6 months in patients with ECV greater than 0.40% but not with ECV less than 0.40%.</p><p><strong>Conclusions and relevance: </strong>This study found that ECV mapping, in systemic AL amyloidosis, is an independent predictor of prognosis, can help define the hematological response associated with better long-term outcomes for each patient and potentially inform treatment strategies.</p>","PeriodicalId":14657,"journal":{"name":"JAMA cardiology","volume":" ","pages":"982-989"},"PeriodicalIF":14.1000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11339700/pdf/","citationCount":"0","resultStr":"{\"title\":\"Redefining Cardiac Involvement and Targets of Treatment in Systemic Immunoglobulin AL Amyloidosis.\",\"authors\":\"Aldostefano Porcari, Ambra Masi, Ana Martinez-Naharro, Yousuf Razvi, Rishi Patel, Adam Ioannou, Muhammad U Rauf, Giulio Sinigiani, Brendan Wisniowski, Stefano Filisetti, Jasmine Currie-Cathey, Sophie O'Beara, Tushar Kotecha, Dan Knight, James C Moon, Gianfranco Sinagra, Ruta Virsinskaite, Janet Gilbertson, Lucia Venneri, Aviva Petrie, Helen Lachmann, Carol Whelan, Peter Kellman, Sriram Ravichandran, Oliver Cohen, Shameem Mahmood, Charlotte Manisty, Philip N Hawkins, Julian D Gillmore, Ashutosh D Wechalekar, Marianna Fontana\",\"doi\":\"10.1001/jamacardio.2024.2555\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Cardiac amyloid infiltration is the key determinant of survival in systemic light-chain (AL) amyloidosis. Current guidelines recommend early switching therapy in patients with a nonoptimal or suboptimal response regardless of the extent of cardiac amyloid infiltration.</p><p><strong>Objective: </strong>To assess the differences between serum biomarkers, echocardiography, and cardiovascular magnetic resonance (CMR) with extracellular volume (ECV) mapping in characterizing cardiac amyloid, the independent prognostic role of these approaches, and the role of ECV mapping to guide treatment strategies.</p><p><strong>Design, setting, and participants: </strong>Consecutive patients newly diagnosed with systemic AL amyloidosis (2015-2021) underwent echocardiography, cardiac biomarkers, and CMR with ECV mapping at diagnosis. Data were analyzed from January to June 2024.</p><p><strong>Main outcomes and measures: </strong>The primary outcomes of the study were all-cause mortality and hematological response as defined according to validated criteria: no response (NR), partial response (PR), very good partial response (VGPR), and complete response (CR). Secondary outcomes were the depth and speed of hematological response and overall survival according to ECV.</p><p><strong>Results: </strong>Of 560 patients with AL amyloidosis, the median (IQR) age was 68 years (59-74 years); 346 patients were male (61.8%) and 214 female (38.2%). Over a median (IQR) 40.5 months 9-58 months), ECV was independently associated with mortality. In the landmark analysis at 1 month, long-term survival was independent of the achieved hematological response in ECV less than 0.30% and ECV of 0.31% to 0.40%, while it was dependent on the depth of the hematological response in ECV greater than 0.40%. In the landmark analysis at 6 months, survival was independent of the achieved hematological response in ECV less than 0.30% and dependent on achieving at least PR in ECV of 0.31% to 0.40%. Survival was dependent on achieving CR in ECV of 0.41% to 0.50% and ECV greater than 0.50%. Achieving a deep hematological response at 1 month was associated with better survival compared with 6 months in patients with ECV greater than 0.40% but not with ECV less than 0.40%.</p><p><strong>Conclusions and relevance: </strong>This study found that ECV mapping, in systemic AL amyloidosis, is an independent predictor of prognosis, can help define the hematological response associated with better long-term outcomes for each patient and potentially inform treatment strategies.</p>\",\"PeriodicalId\":14657,\"journal\":{\"name\":\"JAMA cardiology\",\"volume\":\" \",\"pages\":\"982-989\"},\"PeriodicalIF\":14.1000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11339700/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1001/jamacardio.2024.2555\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamacardio.2024.2555","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Redefining Cardiac Involvement and Targets of Treatment in Systemic Immunoglobulin AL Amyloidosis.
Importance: Cardiac amyloid infiltration is the key determinant of survival in systemic light-chain (AL) amyloidosis. Current guidelines recommend early switching therapy in patients with a nonoptimal or suboptimal response regardless of the extent of cardiac amyloid infiltration.
Objective: To assess the differences between serum biomarkers, echocardiography, and cardiovascular magnetic resonance (CMR) with extracellular volume (ECV) mapping in characterizing cardiac amyloid, the independent prognostic role of these approaches, and the role of ECV mapping to guide treatment strategies.
Design, setting, and participants: Consecutive patients newly diagnosed with systemic AL amyloidosis (2015-2021) underwent echocardiography, cardiac biomarkers, and CMR with ECV mapping at diagnosis. Data were analyzed from January to June 2024.
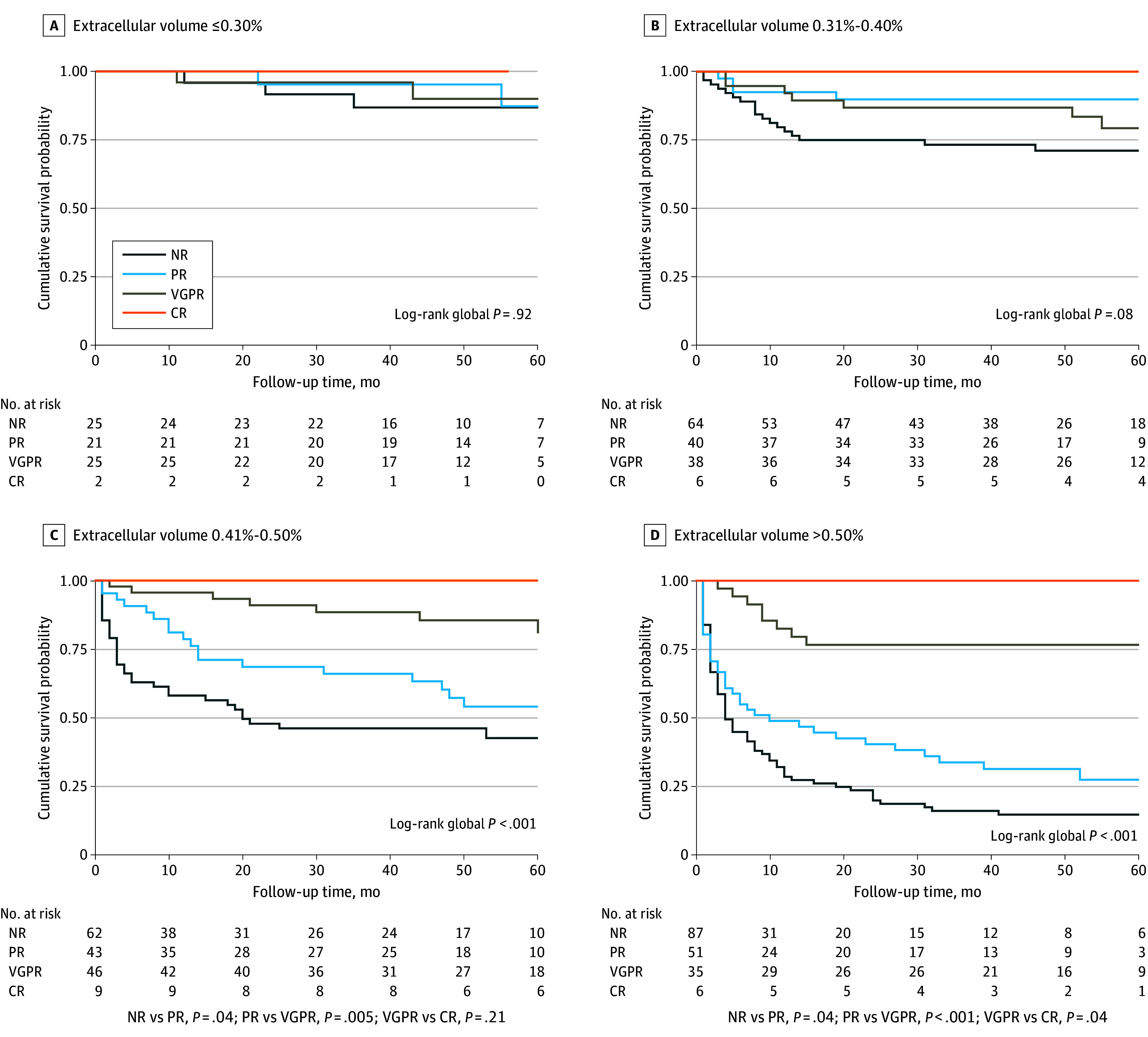
Main outcomes and measures: The primary outcomes of the study were all-cause mortality and hematological response as defined according to validated criteria: no response (NR), partial response (PR), very good partial response (VGPR), and complete response (CR). Secondary outcomes were the depth and speed of hematological response and overall survival according to ECV.
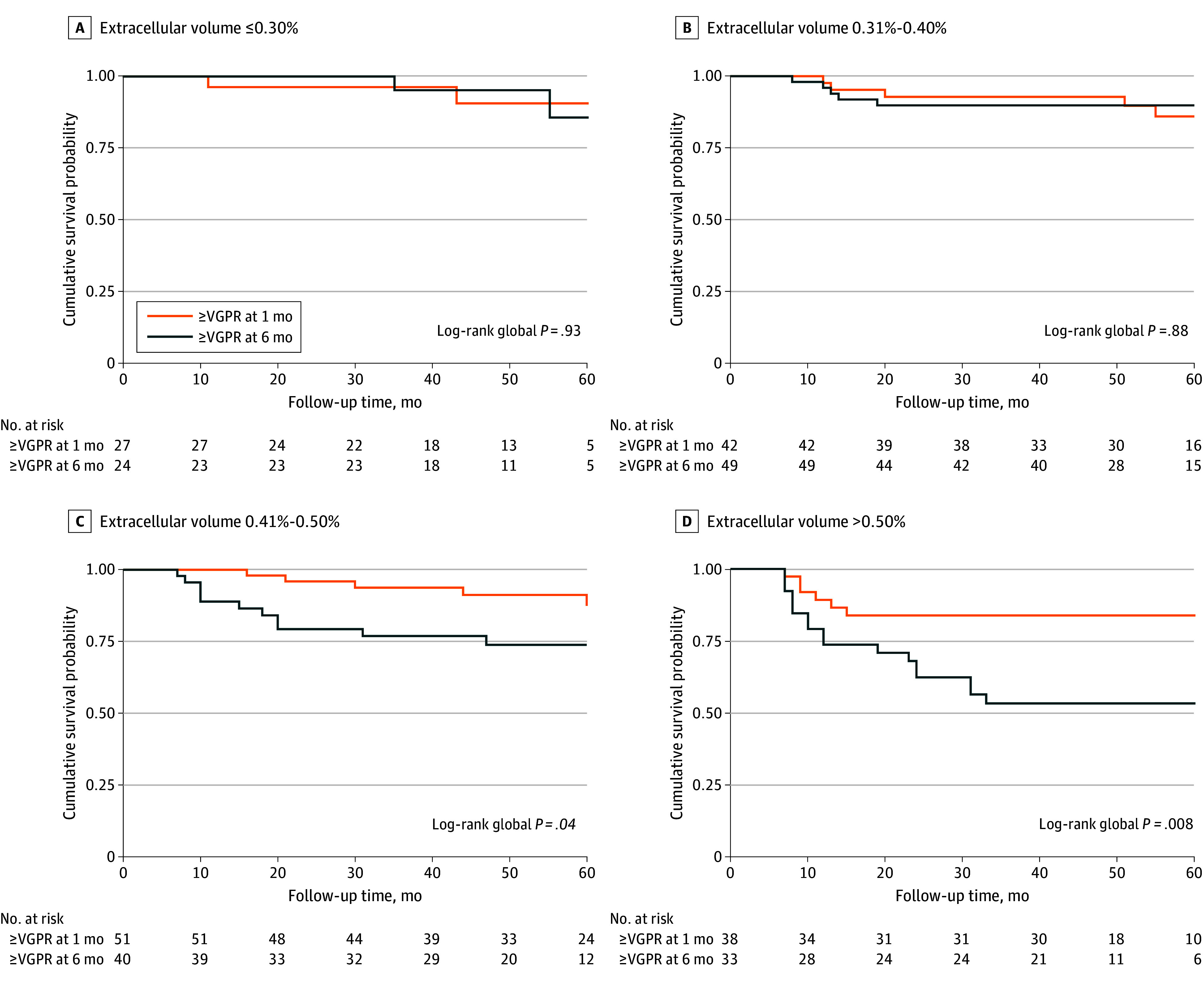
Results: Of 560 patients with AL amyloidosis, the median (IQR) age was 68 years (59-74 years); 346 patients were male (61.8%) and 214 female (38.2%). Over a median (IQR) 40.5 months 9-58 months), ECV was independently associated with mortality. In the landmark analysis at 1 month, long-term survival was independent of the achieved hematological response in ECV less than 0.30% and ECV of 0.31% to 0.40%, while it was dependent on the depth of the hematological response in ECV greater than 0.40%. In the landmark analysis at 6 months, survival was independent of the achieved hematological response in ECV less than 0.30% and dependent on achieving at least PR in ECV of 0.31% to 0.40%. Survival was dependent on achieving CR in ECV of 0.41% to 0.50% and ECV greater than 0.50%. Achieving a deep hematological response at 1 month was associated with better survival compared with 6 months in patients with ECV greater than 0.40% but not with ECV less than 0.40%.
Conclusions and relevance: This study found that ECV mapping, in systemic AL amyloidosis, is an independent predictor of prognosis, can help define the hematological response associated with better long-term outcomes for each patient and potentially inform treatment strategies.
JAMA cardiologyMedicine-Cardiology and Cardiovascular Medicine
CiteScore
45.80
自引率
1.70%
发文量
264
期刊介绍:
JAMA Cardiology, an international peer-reviewed journal, serves as the premier publication for clinical investigators, clinicians, and trainees in cardiovascular medicine worldwide. As a member of the JAMA Network, it aligns with a consortium of peer-reviewed general medical and specialty publications.
Published online weekly, every Wednesday, and in 12 print/online issues annually, JAMA Cardiology attracts over 4.3 million annual article views and downloads. Research articles become freely accessible online 12 months post-publication without any author fees. Moreover, the online version is readily accessible to institutions in developing countries through the World Health Organization's HINARI program.
Positioned at the intersection of clinical investigation, actionable clinical science, and clinical practice, JAMA Cardiology prioritizes traditional and evolving cardiovascular medicine, alongside evidence-based health policy. It places particular emphasis on health equity, especially when grounded in original science, as a top editorial priority.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


